
More Information
Submitted: 11 November 2019 | Approved: 22 November 2019 | Published: 25 November 2019
How to cite this article: Elangovan R, Theyagarajan R, Mani E, Amaladhas MM. Lateral Pedicle and Connective Tissue Graft – A combined approach for management of isolated gingival recession. J Clin Adv Dent. 2019; 3: 023-026.
DOI: 10.29328/journal.jcad.1001012
ORCiD: orcid.org/0000-0003-2399-2658
Copyright License: © 2019 Elangovan R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Gingival recession; Connective tissue graft; Lateral pedicle flap

Lateral Pedicle and Connective Tissue Graft – A combined approach for management of isolated gingival recession
Ramnath Elangovan1*, Ramakrishnan Theyagarajan2, Ebenezer Mani3 and Mejalla Muthiah Amaladhas1
13rd Year Post Graduate Student, Department of Periodontics, Adhiparasakthi Dental College and Hospital, Melmaruvathur, Kanchipuram, India
2Professor, Head of the Department, Department of Periodontics, Adhiparasakthi Dental College and Hospital, Melmaruvathur, Kanchipuram, India
3Reader, Department of Periodontics, Adhiparasakthi Dental College and Hospital, Melmaruvathur, Kanchipuram, India
*Address for Correspondence: Alfred Seban, Head of Department of Oral Surgery, Fondation A de Rotschild, Paris, France, Email: [email protected]
Gingival recession is defined as apical migration of the gingival epithelium leading to the exposure of root surface. There are many surgical procedures for treating gingival recessions and the main goal is to cover the exposed tooth surface by soft tissue augmentation. The surgical techniques performed for root coverage has their own advantages and limitations. The surgical technique used for managing the gingival recession is the major factor that determines the outcome and the long term result of the procedure. The most common surgical technique in treating the isolated gingival recession is the lateral pedicle graft and the surgical technique with highest percentage of root coverage is the connective tissue graft. This case report deals with the management of an isolated gingival recession with lateral pedicle and connective tissue graft. The outcome of the procedure was excellent having complete root coverage.
The apical migration of the gingival epithelium leading to the exposure of the root surface is termed as Gingival Recession. The gingival recession has various etiological factors and the treatment of gingival recession should eliminate the etiological factors followed by achieving the root coverage. Gingival recession may lead to plaque and calculus accumulation, loss of aesthetics, root caries, abrasion of the root surfaces and hypersensitivity. There are many surgical procedures which has been used in management of gingival recessions and technique has their own advantages and limitations. Grupe and Warren described the Lateral Sliding Flap [1]. Presence of adequate amount of soft tissue and the underlying bone at the donor site makes the prognosis of lateral sliding flap good. The major disadvantage of the lateral sliding flap is the formation of gingival defects on the donor tooth. Sullivan and Atkins described the possibility of attaining root coverage by using free grafts at the site of gingival recessions [2,3]. They described that placement of the graft over the recession site causes some amount of “Bridging” because the survival of a portion of a graft is enhanced by the circulation from the vascular bed of the recipient site. In addition to Bridging, Creeping attachment by the coronal migration of the gingival epithelium occurs. The narrowness of the defects and the presence of interdental bone coronal to the buccal bone favours the coronal migration of the free gingival margin. Langer and Langer reported increase of 2 to 6mm of root coverage by placement of sub-epithelial connective tissue graft. It comprised of free connective tissue graft placed underneath a split thickness flap without making any attempt to completely cover the exposed connective tissue. This case report highlights the management of a isolated gingival recession using lateral pedicle and connective tissue graft. The post operative results were good achieving 100 percent root coverage without any post operative complications.
A 30 years old female patient reported to the Department of Periodontics with the chief complaint of lowering of gums in the lower front tooth region for past 2 months. The patient had no previous medical history and dental history. On examination Miller’s Class II recession was elicited in 41 (Figure 1). Patient had an inadequate vestibular depth. Patient underwent initial Phase I therapy followed by Vestibuloplasty using 940 nm Diode laser with the power setting of 1W in Gated Pulse mode (Figure 2). Patient was recalled after four weeks for assessment of healing (Figure 3).

Figure 1: Miller’s Class II Recession in 41.
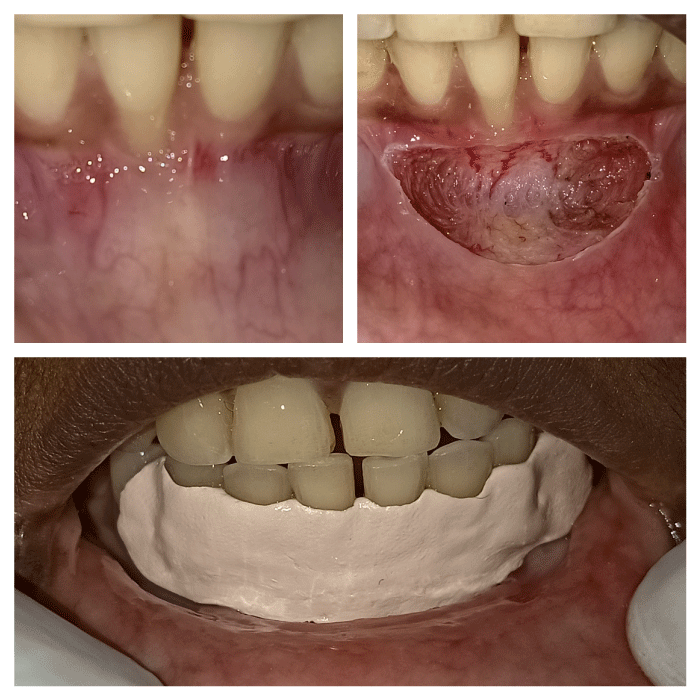
Figure 2: Vestibuloplasty done using 940 nm Diode LASER.
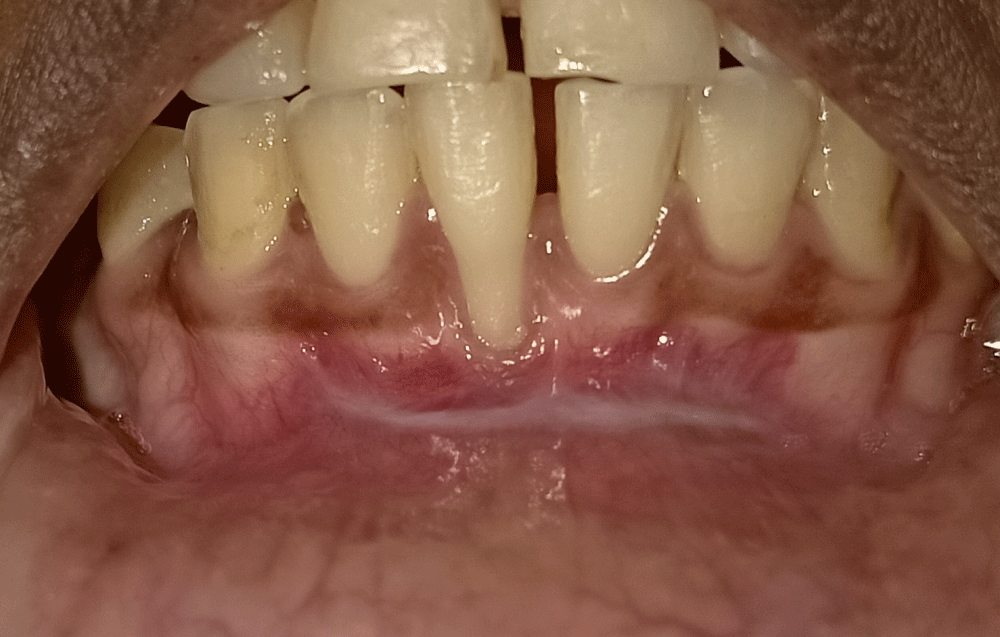
Figure 3: 4 Weeks post operative image after Vestibuloplasty.
Root coverage procedure
Patient was recalled after 4 weeks and assessed for gingival parameters. The parameters such as Pocket depth of about 1mm (Figure 4), Recession Height of about 6mm (Figure 5) and Recession width of about 3mm (Figure 6) was measured pre operatively. Root Coverage was planned using Lateral pedicle Graft combined with Connective tissue graft. After obtaining consent from the patient, the surgical area was anesthetised with Lignocaine (1:2,00,000). Lateral Pedicle graft was reflected from the adjacent tooth 42 (Figure 7). Connective tissue graft was obtained from the palatal surface in relation to 25 and 26, the grafted site was sutured with 3-0 silk suture (Figure 8). The harvested graft was placed over the exposed root surface (Figure 9) and the lateral pedicle graft was placed over the connective tissue graft and secured with 5-0 vicryl independent sutures (Figure 10). Coe-Pak Periodontal dressing was given by placing aluminium foil over the surgical site (Figure 11). Patient was recalled after 1 week for assessment of healing (Figure 12). Three months post operative image showed 100 percent root coverage (Figure 13).
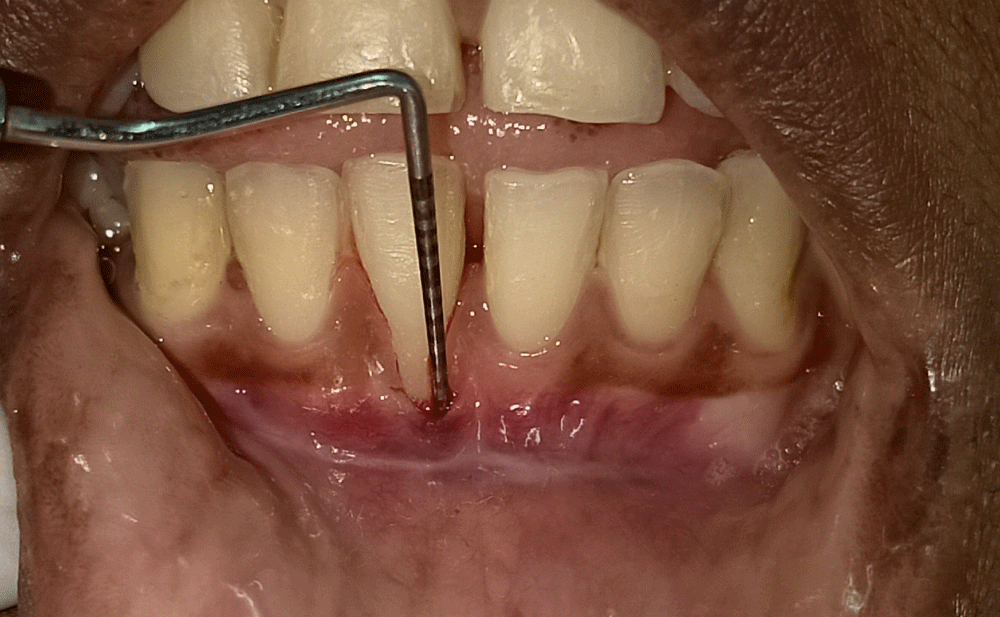
Figure 4:Pocket Depth of 1mm.
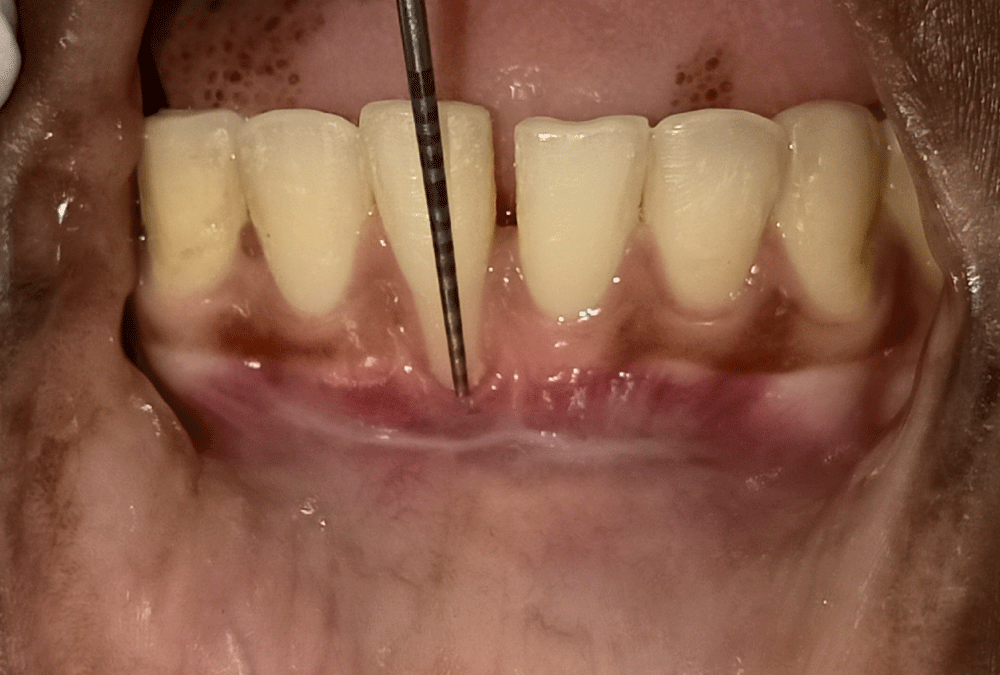
Figure 5: Recession Height of 6mm.
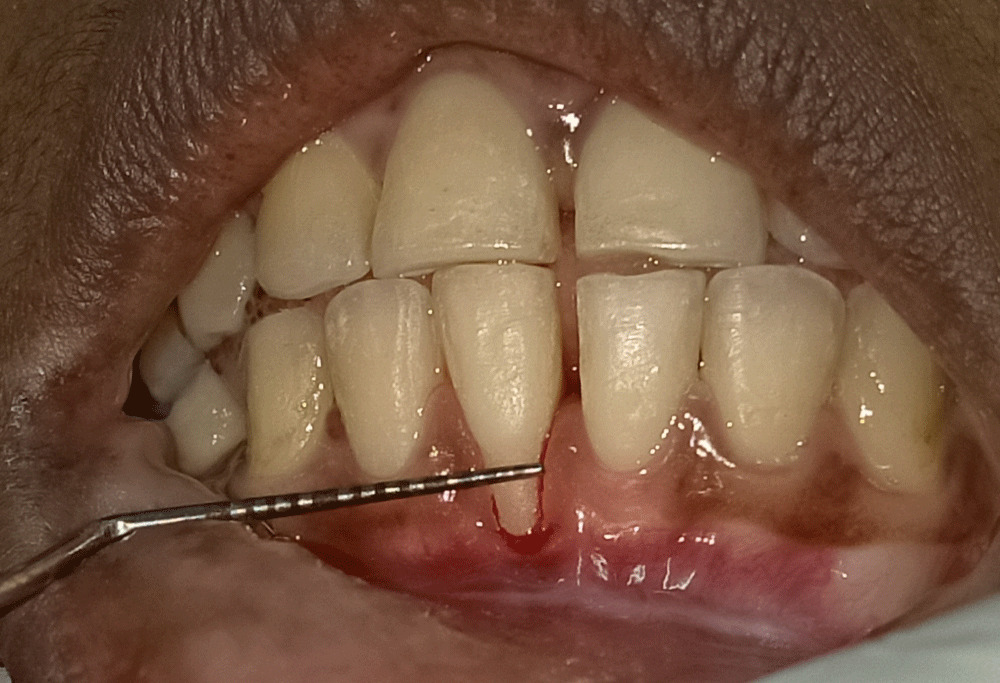
Figure 6: Recession Width of 3mm.

Figure 7: Lateral Pedicle Flap reflected from 42.
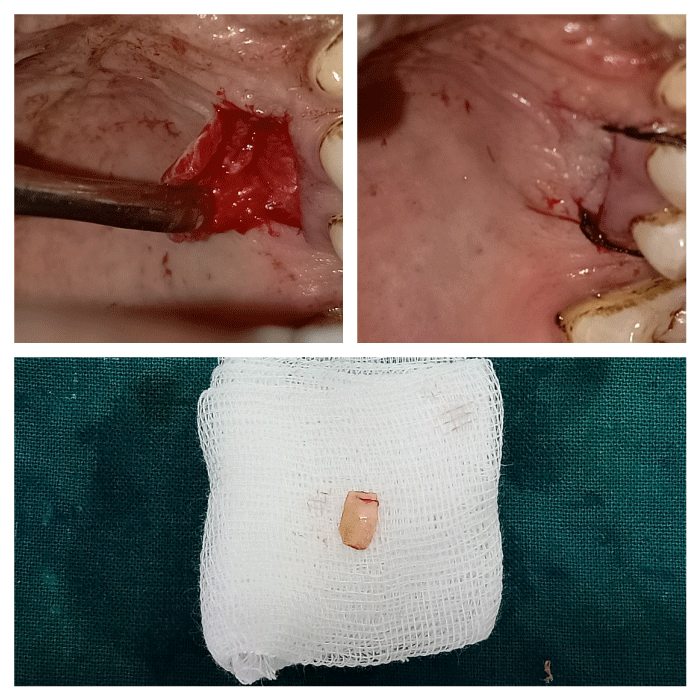
Figure 8: Connective Tissue Graft harvested in relation to Palatal aspect of 25 and 26.
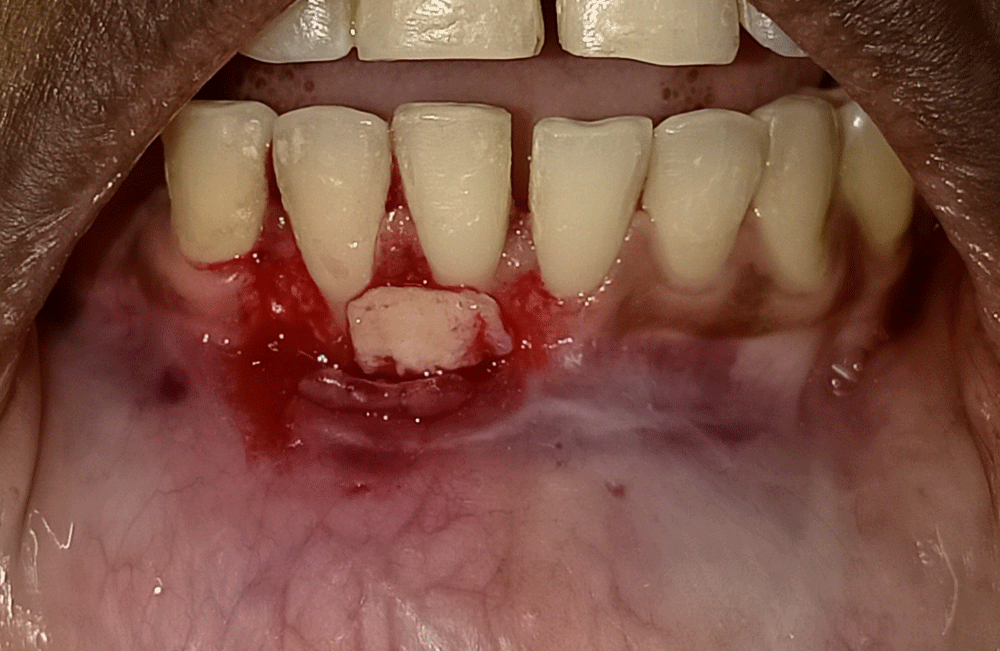
Figure 9: Clinical and panoramic view of implant procedure: The augmented bone remains stable during implant placement the osteosynthesis screw was broken during her removal without any pathological incidence.
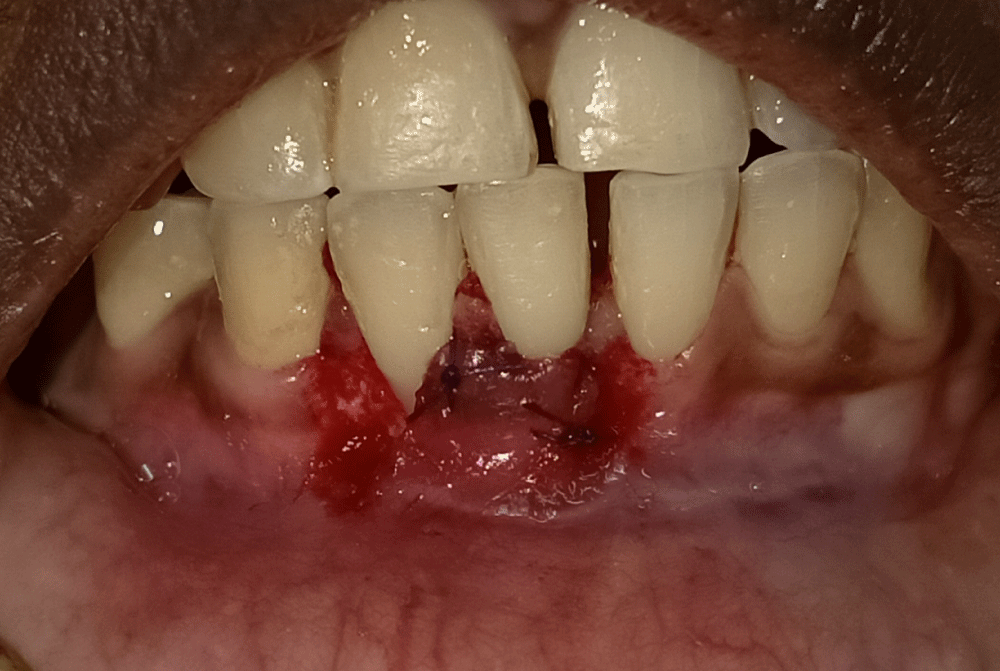
Figure 10: Lateral Pedicle Graft placed over the Connective Tissue Graft and sutured using 5-0 Vicryl suture material.
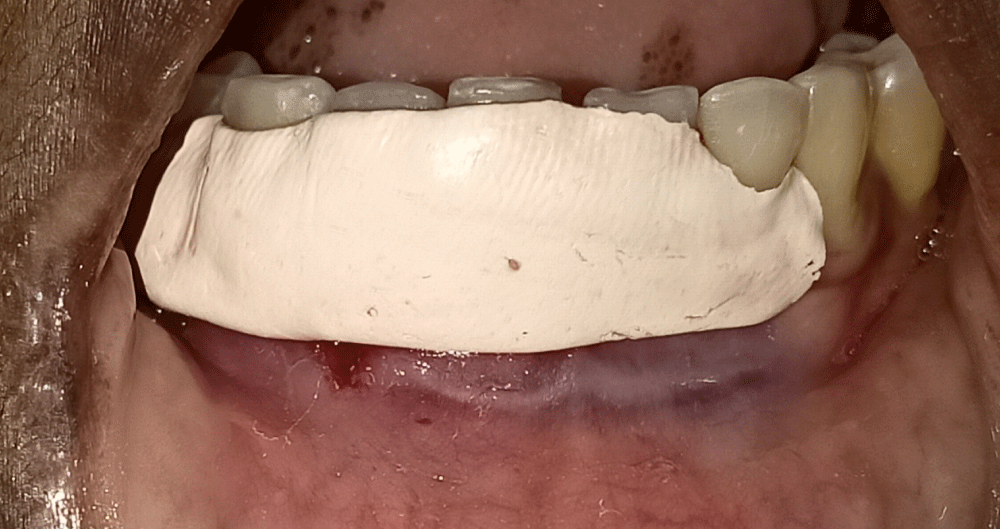
Figure 11: Periodontal dressing placed over the surgical site.

Figure 12: 1 week Postoperative image showing good healing.
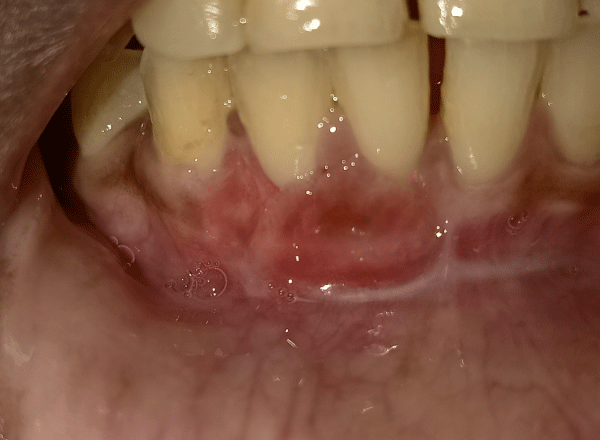
Figure 13: 3 Months postoperative image showing complete root coverage.
There are greater reduction in gingival recession and gain in keratinized tissue when using autogenous connective tissue grafts [4,5]. The surgical technique that is used to treat a recession site depends upon various factors that include the anatomy of the site, width and height of the adjacent keratinized tissue, size of the recession defect, vestibular depth and presence of frenum. Gingival recession may be caused due to many etiological factors. Eliminating the causative factor for the defect should be of priority during treatment planning. In this presented case single isolated recession is due to shallow vestibular depth. Hence, vestibuloplasty was done before root coverage procedure. Studies about percentage of root coverage obtained using various techniques resulted that connective tissue graft along with coronally advanced flap has the highest success rate is about 88% to 98% [6,7]. In the present case scenario there was inadequate keratinized gingiva for obtaining a coronally advanced flap, and there was adequate attached gingiva in the adjacent tooth hence lateral pedicle flap was performed in combination with connective tissue graft. The lateral pedicle graft offers adequate root coverage and survives over the avascular root surface as it retains blood supply from the base. The connective tissue graft provides ensures thickness of the attached gingiva. The outcome of the surgical technique after 3 months showed good results with complete root coverage.
This case report gives a combined technique of covering the denuded root surfaces using subepithelial connective tissue graft and lateral pedicle graft. The graft survives over the denuded root surface as the vascular supply is maintained from the base of the pedicle graft and ensures complete root coverage. The major disadvantage of this technique is that it requires autogenous graft from a secondary donor site which may affect the patient compliance during the surgical procedure. In order to evaluate the efficiency of this combined technique more sample size should be included for the study. Thus combination of lateral pedicle graft and subepithelial connective tissue graft serves as a good technique for the management of isolated gingival recessions.
- Nelson SW. The subpedicle connective tissue graft. A bilaminar reconstructive procedure for the coverage of denuded root surfaces. J Periodontol. 1987; 58: 95-102. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3546673
- Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol. 1985; 56: 715-720. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3866056
- Guinard EA, Caffesse RG. Treatment of localized gingival recessions: Part I. Lateral sliding flap. J Periodontol. 1978; 49: 351-356. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/279662
- Oates TW, Robinson M, Gunsolley JC. Surgical therapies for the treatment of gingival recession. A systematic review. Ann Periodontol. 2003; 8: 303-320. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/14971258
- Prato GP, Tinti C, Vincenzi G, Magnani C, Cortellini P, et al. Guided tissue regeneration versus mucogingival surgery in the treatment of human buccal gingival recession. J Periodontol. 1992; 63: 919-928. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/1453307
- Zucchelli G, Cesari C, Amore C, Montebugnoli L, De Sanctis M. Laterally moved, coronally advanced flap: A modified surgical approach for isolated recession-type defects. J Periodontol. 2004; 75: 1734-1741. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15732880
- Kassab MM, Cohen RE. Treatment of gingival recession. J Am Dent Assoc. 2002; 133: 1499-1506. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12462693