
More Information
Submitted: December 08, 2020 | Approved: December 22, 2020 | Published: December 23, 2020
How to cite this article: Wang CY, Mau JL. Stability of facial soft tissue contour and bone wall at single maxillary tooth gap in early implant placement with contour augmentation: A case report. J Clin Adv Dent. 2020; 4: 030-031.
DOI: 10.29328/journal.jcad.1001022
Copyright License: © 2020 Wang CY, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Stability of facial soft tissue contour and bone wall at single maxillary tooth gap in early implant placement with contour augmentation: A case report
Cheng-Yi Wang1,2 and Jimmy LianPing Mau3-5*
1Department of Dentistry, China Medical University, Taiwan
2Jiaan Dental Clinic, Tainan, Taiwan
3Department of Dentistry, Chi Mei Medical Center, Chiali, Tainan, Taiwan
4Department of Periodontics, Chi Mei Medical Center, Yongkang, Tainan, Taiwan
5Department of Senior Services, Southern Taiwan University of Science and Technology, Taiwan
*Address for Correspondence: Dr. Jimmy LianPing Mau, D.D.S., MS., Department of Dentistry, Chi Mei Medical Center, Chiali, Tainan, Taiwan, Tel: +886-6-2812811; ext. 56056; Fax: +886-6-2523606; Email: [email protected]
Stability of esthetic implant buccal soft and hard tissue contour using freeze-dried bone allograft in early implant placement with contour augmentation.
Early implant placement with contour augmentation using autogenous bone plus deproteinized bovine bone mineral (DBBM) has been documented to rebuild stable facial hard-tissue and soft-tissue contours that are esthetically pleasing [1-4]. For the bone substitute materials, freeze-dried bone allograft (FDBA) has been shown to achieve adequate ridge width during implant placement [5,6]. A comparative randomized study demonstrated autogenous bone plus DBBM and FDBA each combined with a collagen membrane both resulted in a stable implant buccal hard and soft tissue contour in early implant placement with contour augmentation after 1 year [7]. This case report showed stable implant buccal hard and soft tissue contour in early implant placement with contour augmentation using FDBA after 6 years loading.
A 32 years old non-smoking female who denied any systemic disease or drug allergies complaint of biting pain on maxillary anterior region. Clinical examination showed no obvious gingival inflammation and normal probing depth without bleeding on probing. Periapical radiograph showed incomplete PDL lining and radiolucent shadow on tooth 21 root surface, however, a bone sounding examination indicated that buccal crest remained intact. The clinical was diagnosed tooth 21 external root resorption (Figure 1a-c).
Tooth 21 extracted by less traumatic approach using periotome separate circumferential PDL then extract tooth with forcep (Figure 1d) After 8 weeks of healing, a full thickness flap with single vertical release from maxillary canine to canine. Ridge preparation following implant drilling protocol and 4.1 mm x 10 mm Straumann Bone Level implant was placed in ideal 3D position, and cover screw was placed. Freeze-Dried Bone Allograft was placed on top of implant bony defect to augment the buccal contour, then covered with two layers of collagen membrane, primary wound closure was then performed. Wound healing uneventfully during 2-week suture removal (Figure 1e-k).
3-month after implant placement, a small U-shaped flap was performed on top of implant, cover screw was removed, impression was taken at the same time then healing abutment was placed. Two weeks later, implant provisional was performed for implant soft tissue modeling (Figure 1l-o).
Three months after tissue modeling, definitive prosthesis was delivery. Clinical showed stable implant buccal hard and soft tissue contour (Figure 1p,q), 1-year after implant loading, clinical implant buccal hard and soft tissue contour remain stable. Computed tomography also showed stable buccal wall (Figure 1r-t). After 6-year follow up, clinical implant buccal hard and soft tissue contour still remain stable (Figure 1u,v).
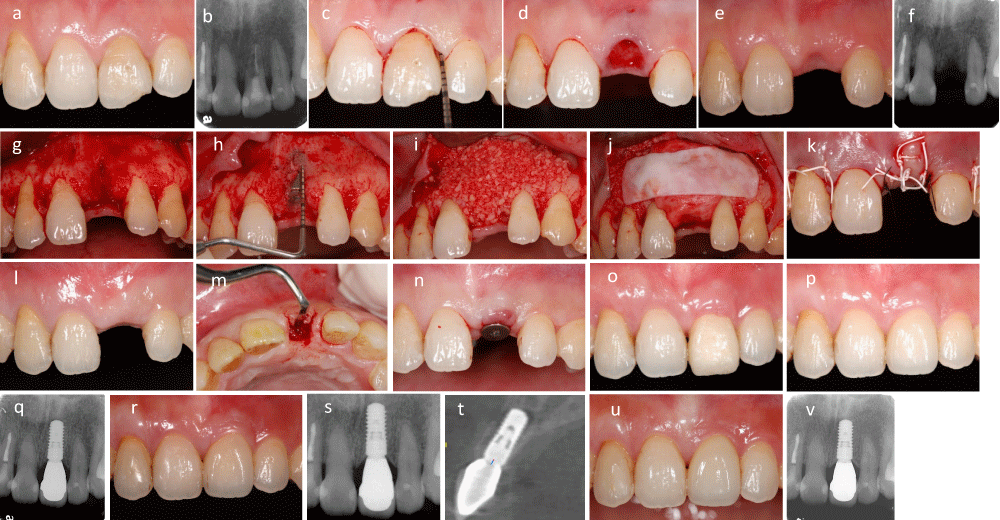
Figure 1: (a,b): Root resorption of tooth 21 was diagnosed, (c): 3 mm bone sounding on buccal and mesiodistal aspect, (d): Less traumatic tooth extraction, (e,f): 2-week after tooth extraction, (g): Full thickness flap elevation, (h): 4.1 mm x10 mm Straumann bone level implant was placed in 3D position, (i-k): Freeze-dried bone allograft placed on the top of implant bony defect, two layers of collagen membrane was covered then primary closure was performed, (l-n): 3-month after implant placement, a U-shaped flap elevation for placement of healing abutment, (o): Provisional soft tissue modeling, (p,q): Final prosthesis delivery, clinical showed esthetic implant buccal hard and soft tissue contour, (r-t): 1-year post loading, clinical implant buccal hard and soft tissue contour remained stable, computed tomographic also showed even buccal bone wall, (u,v): 6-year follow up, clinical implant buccal hard and soft tissue contour still remained stable.
Early implant placement with contour augmentation using FDBA may rebuild stable implant buccal hard and soft tissue contour in long term result.
- Buser D, Halbritter S, Hart C, Bornstein MM, Grütter L, et al. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: 12-month results of a prospective study with 20 consecutive patients. J Periodontol. 2009; 80: 152–162. PubMed: https://pubmed.ncbi.nlm.nih.gov/19228101/
- Buser D, Wittneben J, Bornstein MM, Grutter L, Chappuis V, et al. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. J Periodontol. 2011; 82: 342–349. PubMed: https://pubmed.ncbi.nlm.nih.gov/20831371/
- Buser D, Chappuis V, Kuchler U, Bornstein MM, Wittneben JG, et al. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013; 92: 176S–182S. PubMed: https://pubmed.ncbi.nlm.nih.gov/24158332/
- Chappius V, Rahman L, Buser R, Janner S, Belser U, et al. Long-term effectiveness of contour augmentation with guided bone regeneration: 10-year results. J Dent Res. 2018; 97: 266-274. PubMed: https://pubmed.ncbi.nlm.nih.gov/29073362/
- Feuille F, Knapp CI, Brunsvold MA, Mellonig JT. Clinical and histologic evaluation of bone-replacement grafts in the treatment of localized alveolar ridge defects. Part 1: mineralized freeze-dried bone allograft. Int J Periodontics Restorative Dent. 2003; 23: 29–35. PubMed: https://pubmed.ncbi.nlm.nih.gov/12617366/
- Cammack GV, Nevins M, Clem DS. Histologic evaluation of mineralized and demineralized freeze-dried bone allograft for ridge and sinus augmentations. Int J Periodontics Restorative Dent. 2005; 25: 231–237. PubMed: https://pubmed.ncbi.nlm.nih.gov/16001735/
- Mau JLP, Grodin E, Lin JJ, Chen MCJ, Ho CH, et al. A comparative, randomized, prospective, two-center clinical study to evaluate the clinical and esthetic outcomes of two different bone grafting techniques in early implant placement. J Periodontol. 2019; 90: 247-255. PubMed: https://pubmed.ncbi.nlm.nih.gov/30367723/