
More Information
Submitted: August 23, 2022 | Approved: September 19, 2022 | Published: September 20, 2022
How to cite this article: Alnojaidi S, Samran A, Alyousof D, Jomaa R, Alnojaidi G, et al. Prevalence and awareness of oral habits among adults in Riyadh, Saudi Arabia. J Clin Adv Dent. 2022; 6: 034-040.
DOI: 10.29328/journal.jcad.1001031
Copyright License: © 2022 Alnojaidi S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Adult; Oral; Habit; Nail; Biting

Prevalence and awareness of oral habits among adults in Riyadh, Saudi Arabia
Shahd Alnojaidi1,5, Abdulaziz Samran1,5, Daad Alyousof2, Rahaf Jomaa1,5, Ghadeer Alnojaidi3,5 and Sawsan Alyousef4,5*
1College of Dentistry, Dar Al Uloom University, Saudi Arabia
2Dentistry Department, King Salman Armed Forces Hospital, Tabuk, Saudi Arabia
3College of Medicine, Dar Al Uloom University, Saudi Arabia
4Critical Care Medicine, King Fahad Medical City, Saudi Arabia
5Riyadh, Saudi Arabia
*Address for Correspondence: Sawsan Alyousef, King Fahad Medical City, Saudi Arabia, Email: [email protected]
Introduction: Oral habit is common in childhood and it is proven to cause multiple adverse effects on oral and general health, while oral habits in the adult population are under looked. The prevalence of oral habits varied among different societies. The extent of these effects varies depending on a wide range of variables including the actual habit, the duration, and the intensity of the oral habit.
Objectives: The primary objective is to determine the prevalence of oral habits in adults in Riyadh, Saudi Arabia, and the secondary objective is awareness of different types of oral habits and their adverse effects.
Methods: Descriptive cross-sectional study using questionnaire through google form which will address the prevalence of 5 Oral habits in the adult population, Riyadh, Saudi Arabia such as nail biting, chewing on pens/pencils/Miswak, using the teeth as a tool, chewing ice, and teeth clenching/grinding and bruxism. Also, it will address the awareness of these 5 oral habits and their adverse effects on oral health and prevention modalities.
Results: There were 220 participants. The majority were Saudi (52.7%), females (83.2%) with bachelor’s degrees (63.6%) and around fifty percent with age below 30 years old. The most prevalent pattern was using teeth as a tool (46.8%), followed by chewing ice (43.6%) and nail-biting (39.1%). All five habits were mainly started in childhood; however, a respectable percentage of beginning is still reported during adulthood, particularly for clenching/grinding/ bruxism and chewing ice, with a ratio of 36.4% and 25%, respectively. Most participants who reported clenching/grinding/ bruxism and nail-biting were related to stress (75.3%, 48.8%, respectively). The majority reported that oral habits could harm teeth (82.3%) and could be preventable (78.6%).
Discussion: Most of the studies concentrate on oral habits in children while few studies had concentrated on oral habits in adults. Oral habit is not uncommon in adults, they have either to continue childhood bad habits or practice new oral habit. The adverse effect varies widely on oral and general health. Although the adult population is aware of these side effects few only seek medical advice.
Conclusion: In Saudi Arabia, oral habit is not uncommon in adults. So the recommendation for the prevention of oral habits is to embed it in all public services, at strategic and operational levels.
The teeth play an important role in our physical health and bodily functions. They help us chew food properly so that it can be easily digested and absorbed by our bodies, enable speech and correct pronunciation of words, and enhance our facial structure. The prevalence of oral habits varied among different societies. The extent of these effects varies depending on a wide range of variables including the actual habit, the duration and intensity of the habit, and the inherent dental and skeletal relationship [1]. These habits disrupt muscular balance and bone growth, producing changes in the dental arch, occlusion, Temporomandibular Dysfunction (TMD), speech, and esthetics besides adverse effects on general health as dissemination of infections [2]. Most of the literature concentrates on oral habits for children but unfortunately, adult people have either to continue childhood bad habits or practice new oral habit that is damaging their teeth. There are several oral habits for the adult age group, among these oral habits are nail-biting, chewing on pens/pencils/Miswak, using the teeth as a tool, chewing ice, teeth clenching/grinding and bruxism, and many others. Many people place their smiles in harm’s way on a daily basis and they often don’t even realize they’re endangering their dental health, Plus the cost, time, and resource implications of the treatment of the adverse reactions caused by prolonged oral habits are significantly high. For these reasons we will discuss 5 oral habits in the adult age group: such as nail biting, chewing on pens/pencils/Miswak, using the teeth as a tool, chewing ice, teeth clenching/grinding and bruxism and search for the prevalence of these oral habits and the awareness among adult population in Riyadh, Saudi Arabia.
The primary objective is to determine the prevalence of oral habits in adults in Riyadh, Saudi Arabia, and the secondary objective is awareness of different types of oral habits and their adverse effects.
A descriptive cross-sectional study using questioner through google Forms will address initially the demographic data including age, gender, education level, and nationality. Followed by the prevalence of 5 Oral habits in the adult population, Riyadh, Saudi Arabia such as nail biting, chewing on pens/pencils/Miswak, using the teeth as a tool, chewing ice, teeth clenching/grinding, and bruxism. Each habit has similar questions including Age at onset, age when stopped, frequency, does it is related to stress, any noticed adverse effect on your teeth, any noticed adverse effect on your general health, seek dental/medical advice, did you try to stop it and any family history of similar habit. Also, it will address the awareness of these 5 oral habits and their adverse effects on oral health and prevention modalities (Appendix A)
.Inclusion criteria: Adult population from Riyadh, Saudi Arabia, had experienced one or more oral habits such as (Nail biting, chewing on Pens, Pencils, or Miswak, Using the Teeth as a tool, chewing ice, and Clenching/grinding/bruxism).
Exclusion criteria: Smoking, chronic diseases such as Diabetes mellitus, or malignancy.
Statistical analysis
IBM SPSS Version 22 was used to analyze data. All quantitative data were reported as mean and standard deviations. Qualitative data of nominal and ordinal were reported as frequencies and percentages. Chi-squared Test and Fischer’s-Exact Test were used to determine associations or differences in oral habits with participants’ demographics. Further, a binomial logistic regression was used to determine the independent association between oral habits as general and each specific oral habit (dependent variables) with the demographics (independent variables). Age (> 30 vs. ≤ 30 years old) and level of education (> high school vs. ≤ high school) were recorded as a binomial variable before entering the binomial logistic regression. Finally, all hypotheses were tested as two-sided with a significant p ≤ 0.05
Table 1 shows the demographics of 220 participants. The majority were Saudi (52.7%), females (83.2%) with bachelor’s degrees (63.6%), and around fifty percent with age below 30 years old.
| Table 1: Participants’ demographics (n = 220). | ||
| Variable | n (%) | |
| Gender | Female | 183 (83.2) |
| Male | 37 (16.8) | |
| Age (years) | 18-25 | 71 (32.3) |
| 26-30 | 36 (16.4) | |
| 31-35 | 26 (13.2) | |
| 36-40 | 29 (13.2) | |
| ≥ 41 | 55 (25.0) | |
| Education level | < High school | 5 (2.3) |
| High school | 38 (17.3) | |
| Bachelor | 140 (63.6) | |
| Ph.D./Master | 37 (36.8) | |
| Nationality | Saudi | 116 (52.7) |
| Non-Saudi | 104 (47.3) | |
Table 2 provides details about the prevalence of oral habits among the participants. Around two third of participants (76.4%) reported one or more of the screened oral habits. Almost one-fourth of participants (24.1%) reported the presence of one oral habit, and 17.3%, 15.5%, 9.5% and 10% of predicants reported two, three, fourth, or five oral habits, respectively. Concerning specific oral habits, the most prevalent pattern was using teeth as a tool (46.8%), followed by chewing ice (43.6%), and nail-biting (39.1%). Figures 1,2 display the findings for the number of habits and the frequencies for each specific habit.
| Table 2: Prevalence of oral habits (n = 220). | ||
| Variable | n (%) or Mean (±SD) | |
| Oral habits | Yes | 168 (76.4) |
| No | 52 (23.6) | |
| Number of oral habits | 1.93 ± 1.62 | |
| 0 | 52 (23.6) | |
| 1 | 53 (24.1) | |
| 2 | 38 (17.3) | |
| 3 | 34 (15.5) | |
| 4 | 21 (9.5) | |
| 5 | 22 (10.0) | |
| Using of teeth as a tool | Yes | 103 (46.8) |
| No | 117 (53.2) | |
| Chewing ice | Yes | 96 (43.6) |
| No | 124 (56.4) | |
| Nails biting | Yes | 86 (39.1) |
| No | 134 (60.9) | |
| Clenching/grinding/bruxism | Yes | 77 (35.0) |
| No | 143 (65.0) | |
| Chewing pens/pencils/Miswak | Yes | 63 (28.6) |
| No | 157 (71.4) | |
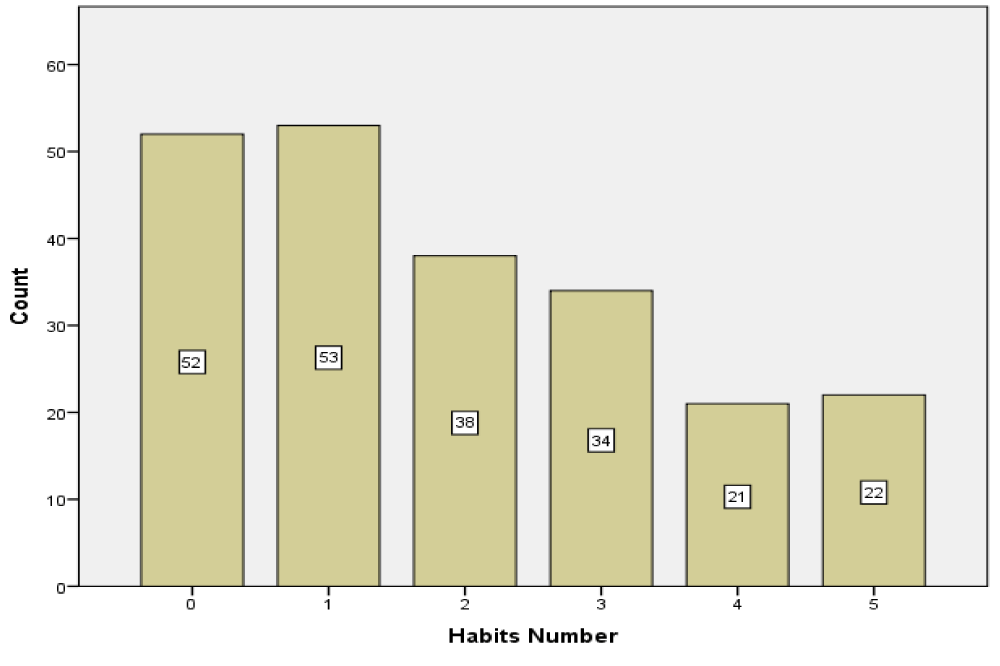
Figure 1: Frequencies for the number of oral habits among the participants.
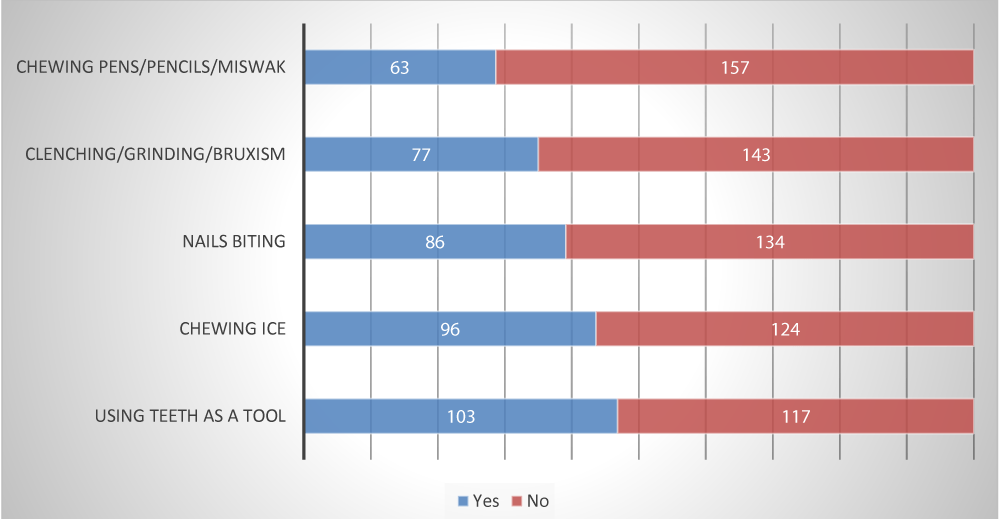
Figure 2: Frequencies of the five oral habits among the participants.
Table 3 provides a detailed description of the five oral habits screened in this study. Concerning the onset of oral habits, it seems that all five habits were mainly started in childhood; however, a respectable percentage of beginning still reported during adulthood, particularly for clenching/grinding/bruxism and chewing ice, with a ratio of 36.4% and 25%, respectively. On the other hand, most oral habits vanished during childhood, except for chewing ice. Interestingly, a respectable percentage of participants still practice the oral habit of clenching/grinding/bruxism (27.3%) and chewing ice (26%). The highest rate of daily practicing oral habits was nail-biting (47.7%) and clenching/grinding/bruxism (37.7%).
| Table 3: Characteristics of oral habits among the participants. | ||||||
| Variable | Oral habits n (%) |
|||||
| Using of teeth as a tool (n = 103) | Chewing ice (n = 96) | Nails biting (n = 86) | Clenching/Grinding/ Bruxism(n = 77) | Chewing pens/pencils/ Miswak(n = 63) | ||
| Age of onset | Childhood | 70 (68.0) | 45 (46.9) | 63 (73.3) | 31 (40.3) | 44 (69.8) |
| Adulthood | 13 (12.6) | 24 (25.0) | 6 (7.0) | 28 (36.4) | 2 (3.2) | |
| Cannot remember | 2 (1.9) | 7 (7.3) | 7 (8.1) | 4 (5.2) | 1 (1.6) | |
| Not reported | 18 (17.5) | 20 (20.8) | 10 (11.6) | 14 (18.2) | 16 (25.4) | |
| Age when stopped | Childhood | 13 (12.6) | 8 (8.3) | 27 (31.4) | 3 (3.9) | 16 (25.4) |
| Adulthood | 29 (28.2) | 16 (16.7) | 21 (24.4) | 14 (18.2) | 19 (30.2) | |
| Cannot remember | 0 (0.0) | 1 (1.0) | 5 (5.8) | 3 (3.9) | 0 (0.0) | |
| Not reported | 38 (36.9) | 46 (47.9) | 24 (27.9) | 36 (46.8) | 21 (33.3) | |
| Not stopped | 23 (22.3) | 25 (26.0) | 9 (10.5) | 21 (27.3) | 7 (11.1) | |
| Frequency | Daily | 15 (14.6) | 12 (12.5) | 41 (47.7) | 29 (37.7) | 18 (28.6) |
| Weekly | 16 (15.5) | 25 (26.0) | 19 (22.1) | 15 (19.5) | 15 (23.8) | |
| Monthly | 12 (11.7) | 15 (15.6) | 4 (4.7) | 8 (10.4) | 5 (7.9) | |
| Rarely | 60 (58.3) | 44 (45.8) | 22 (25.6) | 25 (32.5) | 25 (39.7) | |
| In your opinion, is it related to stress? | Yes | 8 (7.8) | 6 (6.3) | 42 (48.8) | 58 (75.3) | 28 (44.4) |
| No | 80 (77.7) | 80 (83.3) | 13 (15.1) | 4 (5.2) | 19 (30.2) | |
| Maybe | 15 (14.6) | 10 (10.4) | 31 (36.0) | 15 (19.5) | 16 (25.4) | |
| Have you noticed adverse effects on your teeth? | Yes | 32 (31.1) | 30 (31.3) | 17 (19.8) | 45 (58.4) | 14 (22.2) |
| No | 53 (51.5) | 48 (50.0) | 50 (58.1) | 18 (23.4) | 34 (54.0) | |
| Maybe | 18 (17.5) | 18 (18.8) | 19 (22.1) | 14 (18.2) | 15 (23.8) | |
| Have you noticed any adverse effects on your general health? | Yes | 4 (3.9) | 8 (8.3) | 10 (11.6) | 22 (28.6) | 3 (4.8) |
| No | 89 (86.4) | 76 (79.2) | 59 (68.6) | 43 (55.8) | 47 (74.6) | |
| Maybe | 10 (9.7) | 12 (12.5) | 17 (19.8) | 12 (15.6) | 13 (20.6) | |
| Did you seek any medical/dental advice? | Yes | 5 (4.9) | 8 (8.3) | 3 (3.5) | 34 (44.2) | 3 (4.8) |
| No | 97 (94.2) | 87 (90.6) | 81 (94.2) | 42 (54.5) | 57 (90.5) | |
| Maybe | 1 (1.0) | 1 (1.0) | 2 (2.3) | 1 (1.3) | 3 (4.8) | |
| Any attempts of stopping habit? | Yes | 48 (46.6) | 27 (28.1) | 63 (73.3) | 56 (72.7) | 34 (54.0) |
| No | 41 (39.8) | 58 (60.4) | 17 (19.8) | 13 (16.9) | 20 (31.7) | |
| Maybe | 14 (13.6) | 11 (11.5) | 6 (7.0) | 8 (10.4) | 9 (14.3) | |
| Family history of similar habit | Yes | 48 (46.6) | 57 (59.4) | 46 (53.5) | 35 (45.5) | 26 (41.3) |
| No | 37 (35.9) | 25 (26.0) | 26 (30.2) | 22 (28.6) | 24 (38.1) | |
| Maybe | 18 (17.5) | 14 (14.6) | 14 (16.3) | 20 (26.0) | 13 (20.6) | |
Most participants who reported clenching/grinding/ bruxism and nail-biting were related to stress (75.3%, 48.8%, respectively). Further, clenching/grinding/bruxism were the most frequently reported habits that harmed the dental and general health of the participants and were the most frequent habit that got the medical/dental advice. Nails biting and clenching/grinding/bruxism were the most frequently reported habits that got the attention of stopping (73.3% and 72.7%, respectively). Family history of similar habits was common across all five habits, and the highest was chewing ice and biting nails (Table 3).
Table 4 demonstrates participants’ awareness of oral habits. The majority reported that oral habits could harm teeth (82.3%) and could be preventable (78.6%). Teeth damage due to oral habits was the highest adverse effect reported (36.8%).
| Table 4: Participants’ awareness of oral habits (n = 220). | ||
| Variable | n (%) | |
| Can oral habits harm the teeth? | Yes | 181 (82.3) |
| No | 7 (3.2) | |
| Maybe | 32 (14.5) | |
| In your opinion, which of the following adverse effects are caused by oral habits? (Check all that apply) |
The esthetic appearance of your teeth | 63 (33.2) |
| Teeth wear/damage | 81 (36.8) | |
| Speech | 24 (10.9) | |
| Malocclusion | 59 (26.8) | |
| Oral Infection | 41 (18.6) | |
| All the above | 79 (35.98) | |
| None of the above | 15 (6.8) | |
| In your opinion, are oral habits preventable? | Yes | 173 (78.6) |
| No | 7 (3.2) | |
| Maybe | 40 (18.2) | |
Table 5 reported the association between education level and the five oral habits. There were significant relationships between education level and chewing ice (p = 0.001, Fisher’s Exact Test =15.123), as well as education level and clenching/grinding/bruxism (p = 0.016, Fisher’s Exact Test = 9.872).
| Table 5: Crosstabulation of education level and oral habits. | ||||||
| Oral Habits | Education Level | p - value$ | ||||
| < High school | High school | Bachelor | Master/ PhD | |||
| Using of teeth as a tool | Yes | 3 | 18 | 69 | 13 | 0.421 |
| No | 2 | 20 | 71 | 24 | ||
| Chewing ice | Yes | 2 | 17 | 71 | 6 | 0.001* |
| No | 3 | 21 | 69 | 31 | ||
| Nails biting | Yes | 2 | 15 | 59 | 10 | 0.422 |
| No | 3 | 23 | 81 | 27 | ||
| Clenching/grinding/bruxism | Yes | 2 | 6 | 51 | 18 | 0.016* |
| No | 3 | 32 | 89 | 19 | ||
| Chewing pens/pencils/Miswak | Yes | 2 | 9 | 44 | 8 | 0.526 |
| No | 3 | 29 | 96 | 29 | ||
| $ Fisher's Exact Test was used. *p - value ≤ 0.05 (Significant-two sided). | ||||||
Table 6 reported the association between age and the five oral habits. There were significant relationships between age and using teeth as a tool (p = 0.045, χ2 = 9.756) and age and clenching/grinding/bruxism (p = 0.030, χ2 = 10.678). Results for cross-tabulation of gender and nationalities with oral habits were not reported since there were no significant findings. Further, results for cross-tabulation of other demographics with awareness (teeth harm due to oral habits and if the oral habits are preventable) were not reported since there were no significant findings.
| Table 6: Cross tabulation of age and oral habits. | |||||||
| Oral Habits | Age | p - value | |||||
| 18-25 | 26-30 | 31-35 | 36-40 | ≥ 41 | |||
| Using of teeth as a tool | Yes | 40 | 18 | 11 | 7 | 27 | 0.045* |
| No | 31 | 18 | 18 | 22 | 28 | ||
| Chewing ice | Yes | 39 | 17 | 11 | 7 | 22 | 0.060 |
| No | 32 | 19 | 18 | 22 | 33 | ||
| Nails biting | Yes | 38 | 12 | 10 | 9 | 17 | 0.054 |
| No | 33 | 24 | 19 | 20 | 38 | ||
| Clenching/grinding/bruxism | Yes | 18 | 16 | 6 | 11 | 26 | 0.030* |
| No | 53 | 20 | 23 | 18 | 29 | ||
| Chewing pens/pencils/Miswak | Yes | 22 | 9 | 7 | 8 | 17 | 0.929 |
| No | 49 | 27 | 22 | 21 | 38 | ||
| $ Chi-squared test was used. *p - value ≤ 0.05 (Significant-twsided). | |||||||
Table 7 shows the association between oral habits and participants’ demographic through the logistic regression. The multivariate logistic regression shows age and nationality were significantly and independently associated with oral habits while controlling for other factors in the model. Given that other factors were controlled, participants with age ≥ 30 were less likely to practice oral habits than that with age < 30 years old (0.438 (0.223 - 0.857) OR = 0.438, 95% CI: 0.223 - 0.857, p = 0.016). Moreover, non-Saudis were less likely to practice oral habits than participants with negative attitudes (OR = 0.484, 95% CI: 0.294 - 0.941, p < 0.032), given that other factors were controlled. Further detail about each specific health habit is given in Table 7. Finally, binary logistic regression for chewing pens/pencils/Miswak with participants’ demographics was not reported since there were no significant findings.
| Table 7: Results of binary logistic regression analysis of oral habits with participants’ demographics. | |||||
| Variable | Coefficient | Standard error | Wald Test | P -value | OR (95% CI) |
| Oral habits (Present vs. Absent), one or more oral habit | |||||
| Age (> 30 vs. ≤ 30) | -0.827 | 0.343 | 5.799 | 0.016* | 0.438 (0.223-0.857) |
| Education level (> high school vs. ≤ high school) | 0.359 | 0.403 | 0.795 | 0.373 | 1.432 (0.650-3.156) |
| Gender (male vs. female) | 0.111 | 0.449 | 0.061 | 0.804 | 1.118 (0.464-2.693) |
| Nationality (non-Saudi vs. Saudi) | -0.726 | 0.339 | 4.576 | 0.032* | 0.484 (0.294-0.941) |
| Constant | 2.791 | 1.027 | 7.389 | 0.007 | 16.289 |
| Using teeth as a tool (Present vs. Absent) | |||||
| Age (> 30 vs. ≤ 30) | 0.603 | 0.279 | 4.687 | 0.030* | 1.828 (1.059-3.156) |
| Education level (> high school vs. ≤ high school) | 0.103 | 0.349 | 0.088 | 0.767 | 1.109 (0.559-2.198) |
| Gender (male vs. female) | -0.212 | 0.384 | 0.306 | 0.580 | 0.809 (0.381-1.716) |
| Nationality (non-Saudi vs. Saudi) | -0.127 | 0.280 | 0.206 | 0.650 | 0.881 (0.508-1.525) |
| Constant | -0.534 | 0.860 | 0.385 | 0.535 | 0.586 |
| Chewing ice (Present vs. Absent) | |||||
| Age (> 30 vs. ≤ 30) | 0.687 | 0.281 | 5.957 | 0.015* | 1.988 (1.145-3.451) |
| Education level (> high school vs. ≤ high school) | -0.054 | 0.352 | 0.023 | 0.879 | 0.948 (0.475-1.891) |
| Gender (male vs. female) | 0.202 | 0.398 | 0.259 | 0.611 | 1.224 (0.561-2.670) |
| Nationality (non-Saudi vs. Saudi) | 0.327 | 0.284 | 1.323 | 0.250 | 1.386 (0.795-2.419) |
| Constant | -1.394 | 0.884 | 2.483 | 0.115 | 0.248 |
| Nails biting (Present vs. Absent) | |||||
| Age (> 30 vs. ≤ 30) | 0.757 | 0.292 | 6.696 | 0.010* | 2.131 (1.201-3.781) |
| Education level (> high school vs. ≤ high school) | 0.060 | 0.364 | 0.027 | 0.870 | 1.061 (0.520-2.164) |
| Gender (male vs. female) | -0.731 | 0.402 | 3.310 | 0.069 | 0.481 (0.219-1.058) |
| Nationality (non-Saudi vs. Saudi) | 0.666 | 0.296 | 5.057 | 0.025* | 1.946 (1.089-3.477) |
| Constant | -0.912 | 0.888 | 1.056 | 0.304 | 0.402 |
| Clenching/Grinding/ Bruxism (Present vs. Absent) | |||||
| Age (> 30 vs. ≤ 30) | -0.245 | 0.293 | 0.697 | 0.404 | 0.783 (0.441-1.391) |
| Education level (> high school vs. ≤ high school) | -1.026 | 0.426 | 5.808 | 0.016* | 0.358 (0.156-0.826) |
| Gender (male vs. female) | -0.008 | 0.396 | 0.000 | 0.984 | 0.992 (0.457-2.156) |
| Nationality (non-Saudi vs. Saudi) | 0.218 | 0.297 | 0.535 | 0.465 | 1.243 (0.694-2.227) |
| Constant | 2.564 | 1.006 | 6.496 | 0.011 | 12.992 |
| *p - value ≤ 0.05 (Significant-two sided). | |||||
Most of the studies reported a correlation between oral habits and children while only a few studies concentrated on oral habits and adults. Nail biting and thumb sucking are perceived as frequent in many societies [1,2]. Nail Biting (NB) usually does not start until the age of three or four years. The prevalence of NB increases from childhood to adolescence and then decreases in adulthood. The estimated prevalence of nail biting ranges from 20% to 33% in children, however, for teenagers the prevalence is 45%, which tends to decrease after 18 years of age but may persist into adulthood [3]. Motta, et al. found that nail biting is the most prevalent habit (16.4%), and reported a significant association between parafunctional habits and Temporomandibular Dysfunction (TMD) which is more prevalent in cases with bruxism [4]. In Saudi Arabia, the prevalence of nail-biting in the Riyadh region in preschool children and children between the 12 to 16 year age group, is 27% [5,6]. Our study shows 39.1% have nail biting which is the highest among other studies while using the teeth as a tool of 46.8% followed by chewing ice of 43.6% and clenching/grinding/bruxism of 35% and the least is chewing pens/pencils/Miswak with 28.6%. Zakirulla, et al. found that there was a high prevalence of malocclusion associated with harmful oral habits in children among 7 - 13 years in the Aseer region [7]. Adel F. Almutairi, et al. showed similar findings to our study, self-reported parafunctional habits are prevalent in the Saudi adult population, and significantly associated with moderate to severe levels of anxiety, they reported several parafunctional habits including daily gum chewing (86%), lip/object biting (59%), clenching (45%), nail biting (36%) and grinding (32%) [8]. Several studies showed the relation between oral habits and malocclusion which will need extensive orthodontics treatment [9,10]. In our study, the responder’s opinion is nail biting, clenching teeth and chewing pen/pencil and miswak are related to anxiety and stress at 49%, 75%, and 44% respectively, while the minimum correlation between chewing ice, using teeth as a tool with anxiety and stress. Similar studies documented that nail-biting, is a common reaction to stress or anxiety in children and adolescents, a significant positive relationship was observed between the severity of anxiety levels and nail-biting, grinding, clenching, and lip/object biting [11-13].
Nail biting, aside from introducing a host of bacteria into the mouth, places undue pressure on the front teeth, over time, that stress can wear down the tooth enamel, causing chips, breaks, or flattened teeth, this habit is especially risky for people with crowns or veneers because the outer layer porcelain can break off very easily [8]. Chewing on Pens, Pencils, or Miswak can weaken the tooth enamel and lead to chips, cracks, and breaks, these habits may also increase the risk of developing bruxism and gingival recession with extensive use of miswak [14]. Charles Gerba professor of microbiology at the University of Arizona in Tucson showed that a pencil and pencil sharpener carry more bacteria like E. coli and staphylococcus than a toilet seat. American Dental Association had discussed repeatedly the effects of oral habits, using the teeth as a tool: such to remove a nylon string sales tag opening a package, or taking off bottle caps, these actions often lead to a higher risk of cracking the teeth, injuring the jaw or accidentally swallow objects which can necessitate esthetic bonding, a crown, a veneer or worse, extraction of the fractured tooth. Also, Chewing Ice maybe it seems harmless, but biting on cold, hard ice puts the teeth at risk for fractures, cracking, and chipping, and can also cause sharp pains of sensitivity. The fact is when chewing on ice, the enamel on the teeth wears down and the dentin becomes exposed, lastly, clenching/grinding/bruxism can wear teeth down over time. It is most often caused by stress and sleeping habits. Few studies had proved the effectiveness of pre and post-learning at school age and the start of oral treatment early at schools [15,16].
In regards to awareness about the parafunction adverse effect on teeth, several studies found that general awareness of oral health is quite good, where most of the children had a satisfactory understanding of healthy teeth and awareness of parafunction side effects on teeth [17-19]. Similarly, our study demonstrates participants’ awareness of oral habits. The majority reported that oral habits could harm teeth and could be preventable. Teeth damage due to oral habits was the highest adverse effect reported
Oral habit is not uncommon in adults in Saudi Arabia. There are several types of oral habits in the adult population, they have either to continue childhood bad habits or practice new oral habits that are damaging their teeth. In spite, the majority know adverse effects but still practice these habits and it significantly runs in families. These daily habits, if not prevented, can have a long-term impact on the health of the adult population.
Recommendations
The best way to prevent oral habits is to embed it in all public services, at strategic and operational levels such as awareness sessions at schools and universities about the prevention and adverse effects of oral habits. Beside Screening all preliminary, middle, and high school students plus university students to pick up these oral habits and deal with them as early as possible.
- Ghanizadeh A. Association of nail biting and psychiatric disorders in children and their parents in a psychiatrically referred sample of children. Child Adolesc Psychiatry Ment Health. 2008 Jun 2;2(1):13. doi: 10.1186/1753-2000-2-13. PMID: 18513452; PMCID: PMC2435519.
- Ghanizadeh A. Nail biting; etiology, consequences and management. Iran J Med Sci. 2011 Jun;36(2):73-9. PMID: 23358880; PMCID: PMC3556753.
- Marouane O, Ghorbel M, Nahdi M, Necibi A, Douki N. New Approach to Managing Onychophagia. Case Rep Dent. 2016;2016:5475462. doi: 10.1155/2016/5475462. Epub 2016 Nov 23. PMID: 27994890; PMCID: PMC5141299,
- Motta LJ, Guedes CC, De Santis TO, Fernandes KP, Mesquita-Ferrari RA, Bussadori SK. Association between parafunctional habits and signs and symptoms of temporomandibular dysfunction among adolescents. Oral Health Prev Dent. 2013;11(1):3-7. doi: 10.3290/j.ohpd.a29369. PMID: 23507675.
- Aloumi A ,Alqahtani A, Darwish A,Oral parafunctional habits among preschool children in Riyadh, Saudi Arabia, Saudi J. Oral Sci, 5 (1) 2018; 22
- Feteih RM. Signs and symptoms of temporomandibular disorders and oral parafunctions in urban Saudi Arabian adolescents: a research report. Head Face Med. 2006 Aug 16;2:25. doi: 10.1186/1746-160X-2-25. PMID: 16914032; PMCID: PMC1563458.
- Meer Z, Oral Habits: Prevalence and Effects on Occlusion Among 7 to 13 Years Old School Children in Aseer, Saudi Arabia, Pesquisa Brasileira em Odontopediatria e Clínica Integrada · January .2020;DOI: 10.1590/pboci.2020.094
- Almutairi AF, Albesher N, Aljohani M, Alsinanni M, Turkistani O, Salam M. Association of oral parafunctional habits with anxiety and the Big-Five Personality Traits in the Saudi adult population. Saudi Dent J. 2021 Feb;33(2):90-98. doi: 10.1016/j.sdentj.2020.01.003. Epub 2020 Jan 16. PMID: 33551622; PMCID: PMC7848802.
- Frazão P, Narvai PC. Socio-environmental factors associated with dental occlusion in adolescents. Am J Orthod Dentofacial Orthop. 2006 Jun;129(6):809-16. doi: 10.1016/j.ajodo.2004.10.016. PMID: 16769500.
- Fields P JrHW.Contemporary Orthodontics.St.Louis: MosbyInc.2000;134-135.
- Gungormus Z, Erciyas K. Evaluation of the relationship between anxiety and depression and bruxism. J Int Med Res. 2009 Mar-Apr;37(2):547-50. doi: 10.1177/147323000903700231. PMID: 19383250.
- Al-Darwish MS. Oral health knowledge, behaviour and practices among school children in Qatar. Dent Res J (Isfahan). 2016 Jul-Aug;13(4):342-53. doi: 10.4103/1735-3327.187885. PMID: 27605993; PMCID: PMC4993063.
- Leme M, Barbosa T, Castelo P, Gavião MB. Associations between psychological factors and the presence of deleterious oral habits in children and adolescents. J Clin Pediatr Dent. 2014 Summer;38(4):313-7. doi: 10.17796/jcpd.38.4.c48238322205466w. PMID: 25571681.
- Eid MA, Selim HA, al-Shammery AR. The relationship between chewing sticks (Miswak) and periodontal health. 3. Relationship to gingival recession. Quintessence Int. 1991 Jan;22(1):61-4. PMID: 1784721.
- Shivaraju PT, Manu G, Vinaya M, Savkar MK. Evaluating the effectiveness of pre- and post-test model of learning in a medical school. Natl J Physiol Pharm Pharmacol 2017;7(9):947-951.
- Shailee F, Girish M, Kapil R, Nidhi, P. Oral health status and treatment needs among 12- and 15-year-old government and private school children in Shimla city, Himachal Pradesh, India. Journal of International Society of Preventive and Community Dentistry. 2013; 3(1), 44. doi:10.4103/2231-0762.115715
- Wahengbam PP, Kshetrimayum N, Wahengbam BS, Nandkeoliar T, Lyngdoh D. Assessment of Oral Health Knowledge, Attitude and Self-Care Practice Among Adolescents - A State Wide Cross- Sectional Study in Manipur, North Eastern India. J Clin Diagn Res. 2016 Jun;10(6):ZC65-70. doi: 10.7860/JCDR/2016/20693.8002. Epub 2016 Jun 1. PMID: 27504414; PMCID: PMC4963774.
- Al-Darwish MS. Oral health knowledge, behaviour and practices among school children in Qatar. Dent Res J (Isfahan). 2016 Jul-Aug;13(4):342-53. doi: 10.4103/1735-3327.187885. PMID: 27605993; PMCID: PMC4993063.
- Wyne AH, Chohan AN, Al-Dosari K, Al-Dokheil M. Oral health knowledge and sources of information among male Saudi school children. Odontostomatol Trop. 2004 Jun;27(106):22-6. PMID: 15536717.