
More Information
Submitted: August 13, 2022 | Approved: September 21, 2022 | Published: September 27, 2022
How to cite this article: Cresseaux P, Filippi R. A new mandibular anchoring technique. J Clin Adv Dent. 2022; 6: 041-044.
DOI: 10.29328/journal.jcad.1001032
Copyright License: © 2022 Cresseaux P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

A new mandibular anchoring technique
Paul Cresseaux and Raphaël Filippi*
Graduated, Faculty of Lyon, 16 Republic street, 69002, Lyon, France
*Address for Correspondence: Dr. Raphael Filippi, Dental Surgeon, Orthodontist, Graduated, Faculty of Lyon, 16 Republic street, 69002, Lyon, France, Email: [email protected]
Posterior anchorage in the mandible has always been difficult to obtain during our orthodontic treatments. We tried a large number of screw anchors and plate systems which gave us quite acceptable clinical results but had many drawbacks. The retromolar trigonal area presents a thick mucosa and complicated access. The systems are often difficult for orthodontists to use and reactivate. They are inconvenient for patients who are frequently injured, which significantly increases emergency appointments in our offices. Finally, they all require a surgical reoperation at the time of their removal because they are buried to be firmly anchored distal to the mandibular teeth. However, this area is very interesting for orthodontic anchorage because distalizing mandibular molars opens up new avenues in many treatment plans. We were inspired by a technique developed in the 1930s, by Vitali Abalakov, a Soviet mountaineer. He revolutionized mountaineering by developing an infallible anchorage in the ice, which enabled him to achieve many ascents in the Caucasus. This technique, which bears his name, was a real revolution in glacier mountaineering and is still used today. This system is quick to set up, inexpensive (requires only a simple piece of cord), very easy to remove and leaves, in the end, no trace in the ice. It is an anchor of great simplicity since it is only the connection, by a cord, of two holes in the ice that come together. It is extremely reliable thanks to the ice bridge that traps the rope (Figure 1).

Figure 1: Final position of the anchor, front view. The cord is imprisoned by a bridge of ice.
We therefore logically tried to use the brilliant idea of this mountaineer to answer our problems of anchoring posterior to the mandible. We propose in this article a new orthodontic anchorage, which like the Abalakov in the 1930s, will certainly revolutionize dental anchorage. With this technique, posterior mandibular anchorage is now simple, reliable, inexpensive, does not require reoperation, is easily reactivated and above all, is very comfortable. In this article, we present a clinical case where molar distalization and straightening of the mandibular incisors were essential in order to obtain a quality result (Figures 2-5).

Figure 2: Extraoral examination: This adult patient, aged 32, was already treated when she was a teenager. She presented with dental and skeletal class 2 and her orthodontist then extracted four permanent premolars. She now has joint problems with limited mouth opening, a gummy smile and retrogenia. Endoral examination: The intraoral examination shows an incisor overbite, a dento-maxillary disharmony and a correct transverse direction. In the sagittal direction, there is a dental class II.
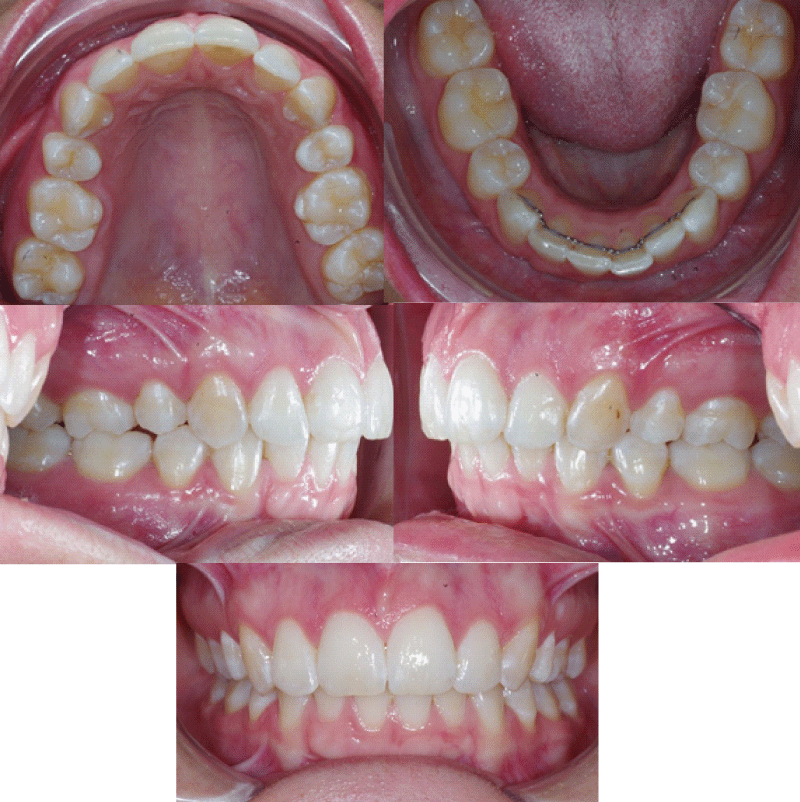
Figure 3: Endoral examination on x-ray examination, it is observed that the wisdom teeth have been removed.

Figure 4: Early treatment orthopantomography. The cephalometric examination confirms the diagnosis of skeletal class II by retromandibularity and the strong vestibulo-version of the mandibular incisors (112°).
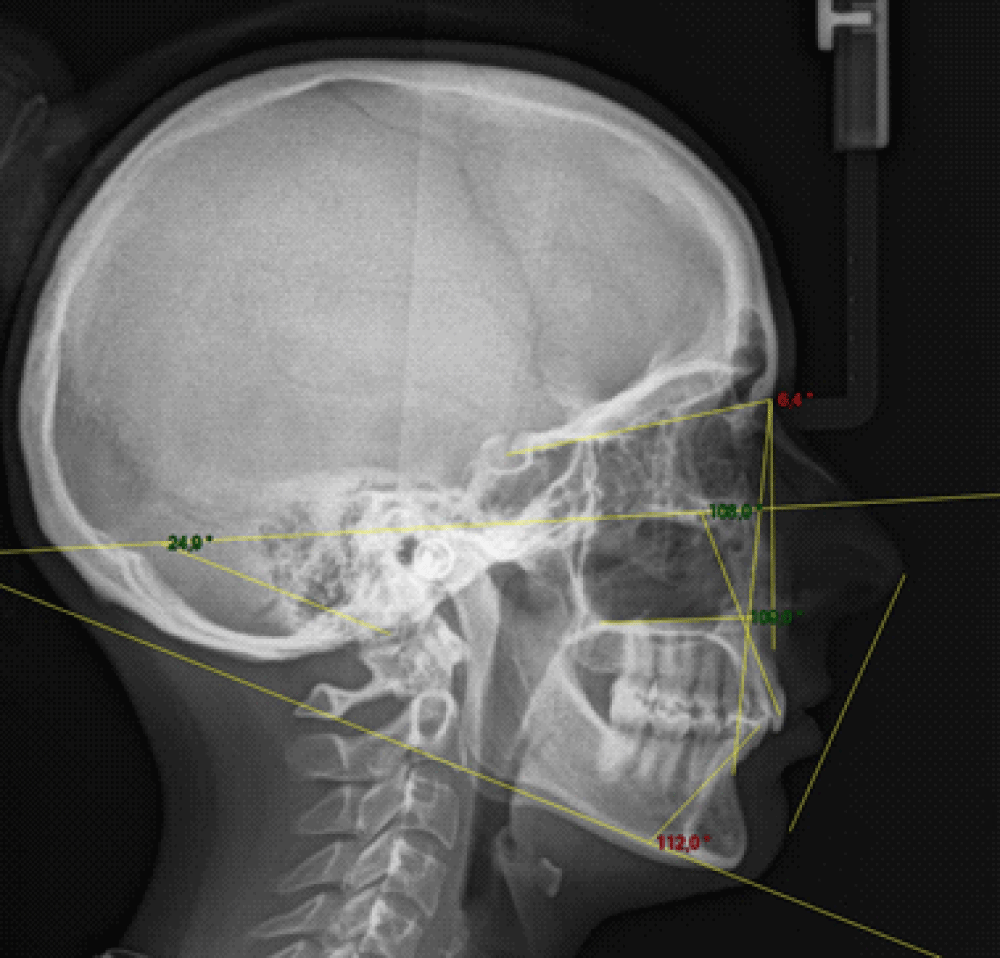
Figure 5: Cephalometric examination at the start of treatment.
The chosen treatment is as follows: An orthodontic-surgical protocol lasting 18 months. We offer Abalakov-type mandibular anchorages to effectively prepare for mandibular advancement by straightening the lower incisor. Our objective is to distalize the molars and find a correct mandibular axis of 90°. This will allow effective mandibular propulsion to correct retrogenia and obtain correct Class I occlusion with standardized dental axes. The patient is fitted by Doctor Raphaël FILIPPI with a self-ligating GC Orthodontics vestibular multi-attachment system in Roth .022 x .028. The first wires put in place are Bio Edge .020 x .020/F200 archwires from GC Orthodontics (shape memory archwires). The mandibular posterior anchorages by osteosynthesis wire are positioned by Dr. Paul CRESSEAUX. The anchors will be placed on the day the attachments are placed and immediately connected to the mandibular canines with 300 gram Nickel-Titanium springs on both sides. An elastic chain is placed from 33 to 43 in order to avoid the appearance of diastemas between the anterior teeth during recoil. The recoil is done en masse without any parasitic effect because the direction of traction is in the axis of the lower wire. The chain will be changed monthly during the patient’s appointments (Figure 6).
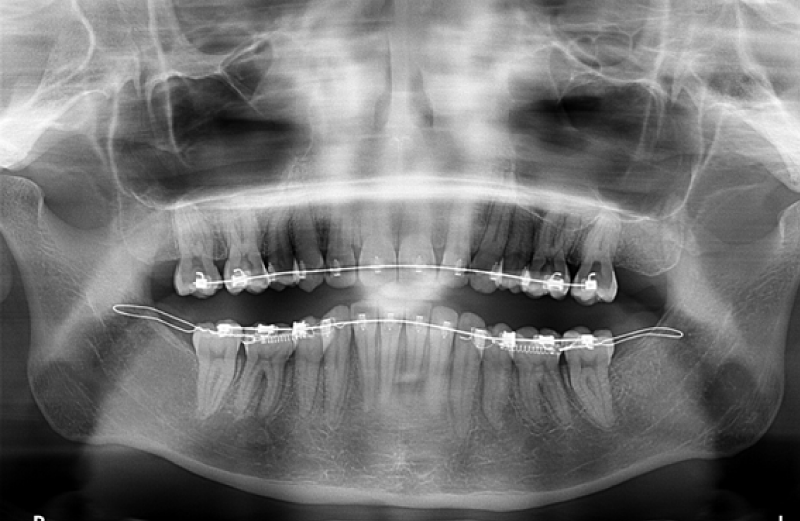
Figure 6: Orthopantomography taken during traction of the system. The springs are connected between the Abalakovs and the mandibular canines in direct traction.
The surgical procedure
We use simple osteosynthesis wires that were used 20 years ago, before the advent of plate osteosynthesis. They are placed opposite half of the molar coronal height, which corresponds to the bonding height of the multi-bracket appliance. These threads can be inserted under local anesthesia (intravenous sedation can complement it). Access to the ascending ramus of the mandible is equivalent to the access achieved for extractions of wisdom teeth. These are also often extracted during the operation, which improves the decline of the lower arch and therefore the incisor straightening. A perforation of the ascending branch is performed, under irrigation, using a round bur mounted on a surgical handpiece, in order to pass the osteosynthesis wire on either side, protecting the lingual nerve. An osteosynthesis wire (4/10th of a mm in diameter) is then inserted into the perforation. The two strands will be twisted and folded at the level of the orthodontic appliance during the surgical procedure so as not to disturb the patient. The traction by the orthodontist can take place quickly after the installation of the system. The post-operative follow-up is simple and most often summarized to that of the extraction of wisdom teeth when they take place at the same time (Figures 7,8).
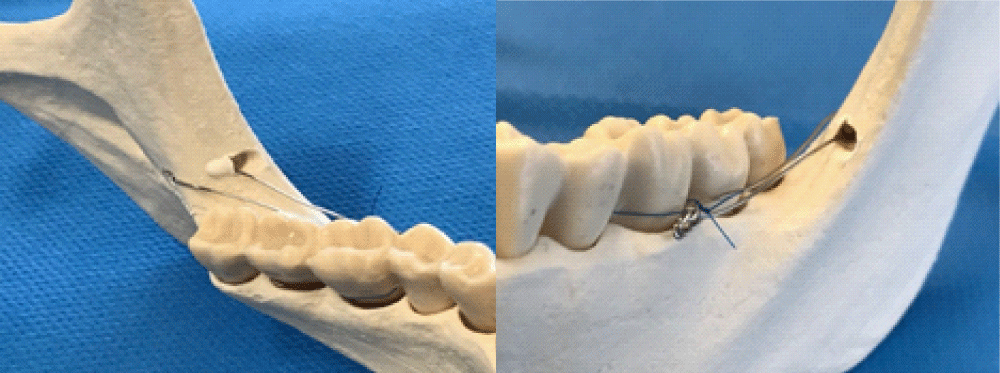
Figure 7: The anchorage is pulled by a 300 gram Nickel-Titanium spring that is simply put in place after the operation. The posterior end of the Nickel-Titanium spring is fixed to the twisted part of the osteosynthesis wire. The anterior end of the spring is connected to the lower multi-ring apparatus by a metal ligature. In this case, it is a direct pull. In the case of our patient, the distalization begins on a shape-memory wire of section .020 x .020.
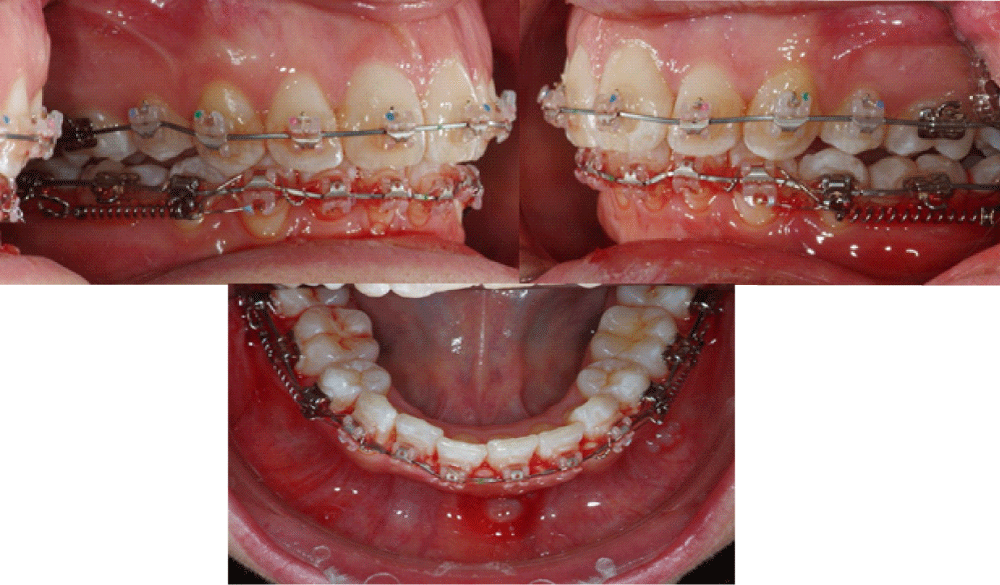
Figure 8: View of the traction system from the right side, left side, then in occlusal view.
The first results are obtained quickly. Traction does not need to be reactivated at each appointment. After 6 months of traction, the desired incisor straightening is obtained and we schedule the mandibular advancement intervention. The comparison of the teleradiographies makes it possible to objectify the mandibular incisor straightening and the mandibular molar distalization obtained. We also observe the maintenance of the incisor axes at the level of the maxillary arch. There is a very significant incisor straightening. Indeed, the mandibular incisor axis went from 112° to 90.3° in 6 months. The maxillary incisor axes were maintained, which corresponds perfectly to our initial orthodontic preparation objective (Figure 9).
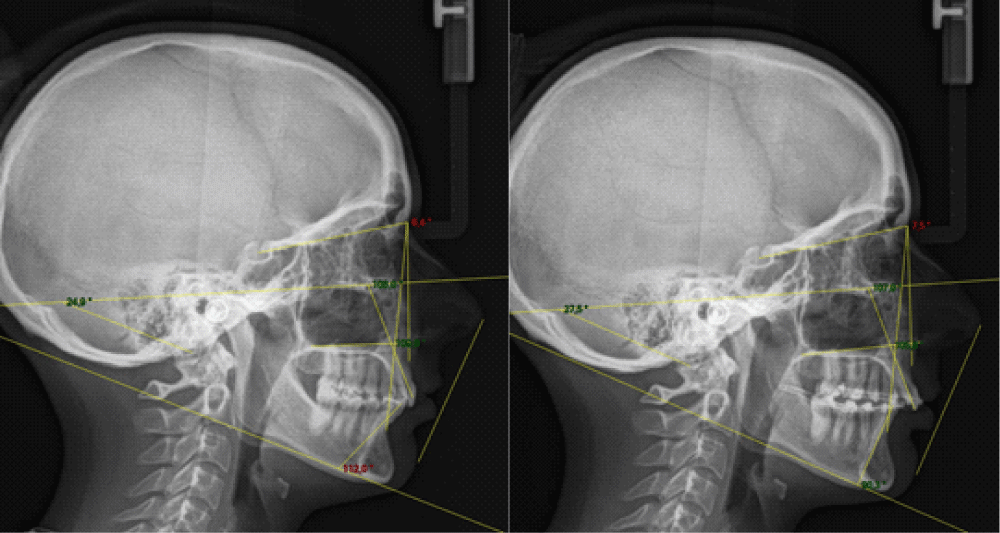
Figure 9:
Lateral cephalograms
Comparison between the image at the start of treatment and the control image after 6 months of traction on the wire anchorage in the ascending mandibular branch. The incisal angle changed from 112° to 90.3°. Throughout the treatment, the patient did not complain of any discomfort due to this traction system and she even described it as “comfortable”. The system was removed during orthognathic surgery. The operation was performed by Dr. Paul CRESSEAUX, during the 7th month of treatment. The intervention consisted of a maxillary expansion in a single operation by a Lefort 1 segmented into two fragments. We had to obtain an expansion of the arch in the posterior sectors of 5mm. Maxillary impaction has been associated with reducing gummy smiling and improving lip proficiency. Mandibular advancement was performed at the same time. Thanks to the good straightening of the incisor axes and therefore to an effective pre-surgical decompensation phase, mandibular advancement could be achieved and made it possible to completely correct the skeletal and dental class II. The pre-surgical decompensation phase was obtained very quickly thanks to our anchorage. The total duration of this orthodontic-surgical treatment was therefore ultimately 15 months. The skeletal, dental and functional objectives were achieved. The patient presents with bilateral mastication at the end of treatment. His joint problems have completely disappeared. She is very satisfied with the aesthetics of her face. His gummy smile has been corrected. Dental decompensation allowed effective mandibular advancement which contributed to excellent correction of retrogenia (Figures 10-13) [1-23].

Figure 10: End of treatment extraoral photos.
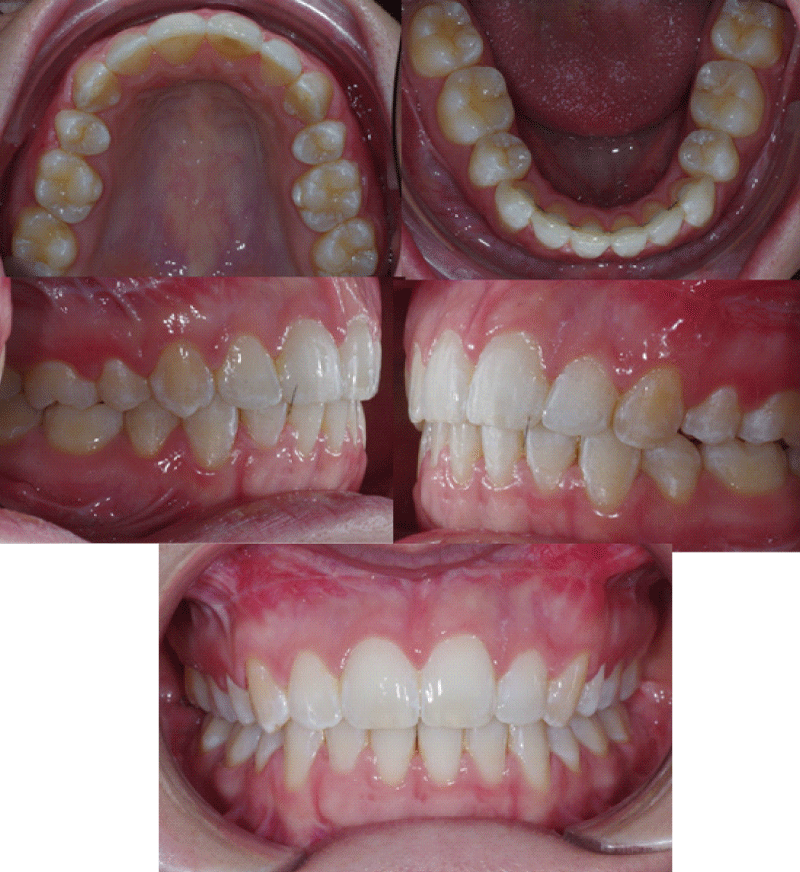
Figure 11: End of treatment intraoral photos.
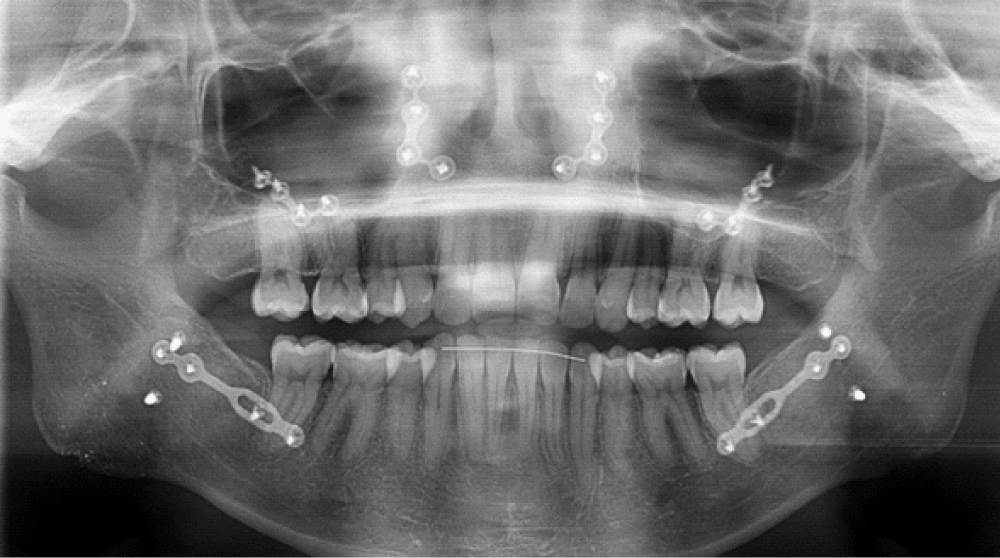
Figure 12: Orthopantomographic examination at the end of treatment.
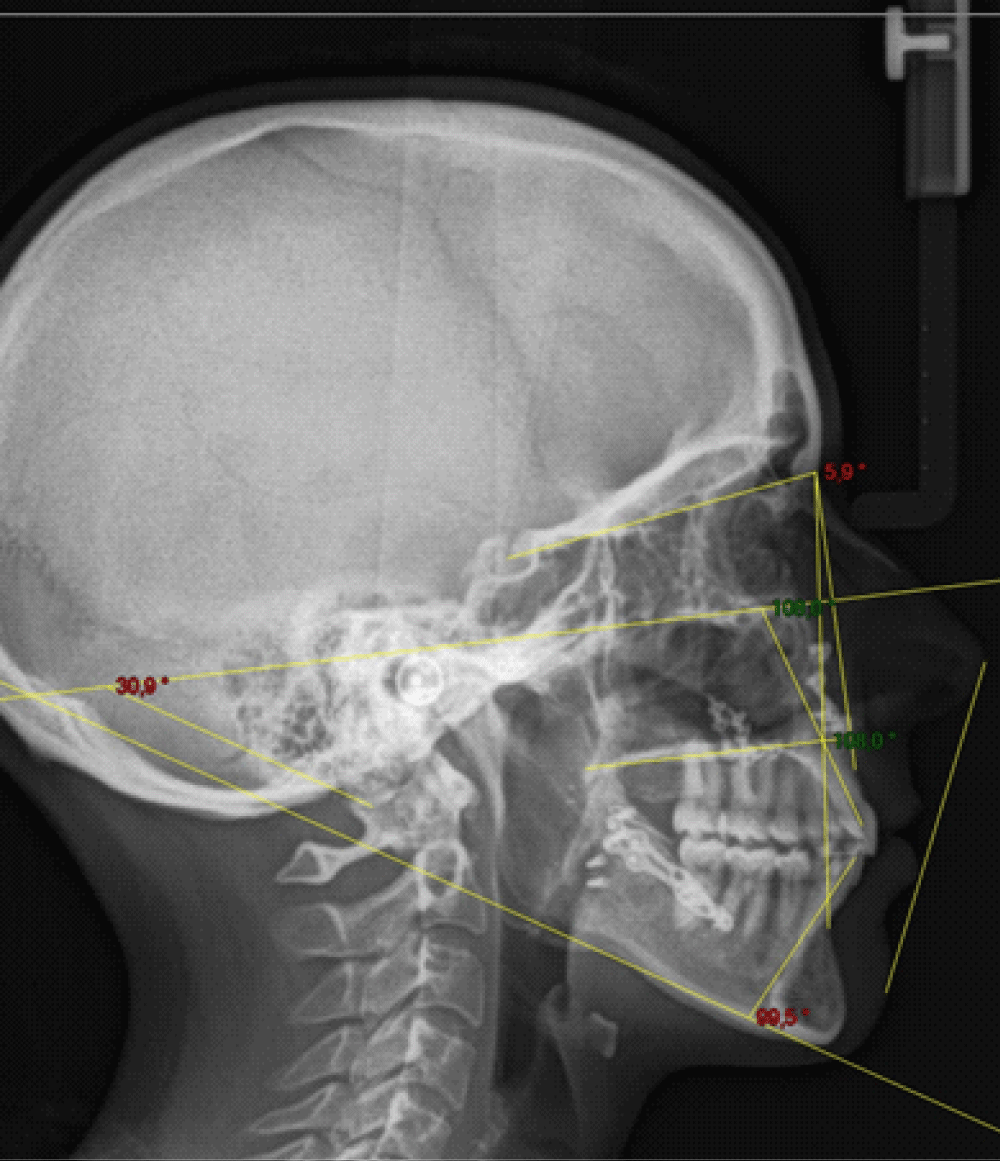
Figure 13: Cephalometric examination at the end of treatment.
Mandibular wire anchorage has taken us into a new dimension of orthodontic anchorage. As often, good ideas come in different areas and the ingenuity of Vitali ABALAKOV has revolutionized our daily orthodontic practice. The distalization of mandibular teeth has become a simple orthodontic option, comfortable for the patients and also for the orthodontist. The results are predictable and the system does not constitute an additional cost for the patient. Orthodontic preparations for mandibular advancement surgeries where significant incisor straightening is necessary can be considered calmly and indications for premolar extractions are becoming rarer. Purely orthodontic corrections of dental class III with receding mandibular teeth will now be approached more simply. We decided by mutual agreement between Doctors Paul Cresseaux and Raphaël Filippi to call this bone anchorage “an ABALAKOV”. Conflicts of interest: the authors declare that they have no conflicts of interest.
- Yu J, Park JH, Bayome M, Kim S, Kook YA, Kim Y, Kim CH. Treatment effects of mandibular total arch distalization using a ramal plate. Korean J Orthod. 2016 Jul;46(4):212-9. doi: 10.4041/kjod.2016.46.4.212. Epub 2016 Jul 25. PMID: 27478798; PMCID: PMC4965592.
- Sugawara J, Daimaruya T, Umemori M, Nagasaka H, Takahashi I, Kawamura H, Mitani H. Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004 Feb;125(2):130-8. doi: 10.1016/j.ajodo.2003.02.003. PMID: 14765050.
- Kook YA, Park JH, Bayome M, Kim S, Han E, Kim CH. Distalization of the mandibular dentition with a ramal plate for skeletal Class III malocclusion correction. Am J Orthod Dentofacial Orthop. 2016 Aug;150(2):364-77. doi: 10.1016/j.ajodo.2016.03.019. PMID: 27476370.
- Bernard-Granger C, Filippi R, Cresseaux P. Quand l’alpinisme vient révolutionner l’ancrage orthodontique. L’orthodontiste. 2017; 6:8.
- Park HS, Lee SK, Kwon OW. Group distal movement of teeth using microscrew implant anchorage. Angle Orthod. 2005 Jul;75(4):602-9. doi: 10.1043/0003-3219(2005)75[602:GDMOTU]2.0.CO;2. PMID: 16097229.
- Oh YH, Park HS, Kwon TG. Treatment effects of microimplant-aided sliding mechanics on distal retraction of posterior teeth. Am J Orthod Dentofacial Orthop. 2011 Apr;139(4):470-81. doi: 10.1016/j.ajodo.2009.05.037. PMID: 21457858.
- Alharbi F, Almuzian M, Bearn D. Miniscrews failure rate in orthodontics: systematic review and meta-analysis. Eur J Orthod. 2018 Sep 28;40(5):519-530. doi: 10.1093/ejo/cjx093. PMID: 29315365.
- Findik Y, Baykul T, Esenlik E, Turkkahraman MH. Surgical difficulties, success, and complication rates of orthodontic miniplate anchorage systems: Experience with 382 miniplates. Niger J Clin Pract. 2017 May;20(5):512-516. doi: 10.4103/1119-3077.187320. PMID: 28513506.
- Lam R, Goonewardene MS, Allan BP, Sugawara J. Success rates of a skeletal anchorage system in orthodontics: A retrospective analysis. Angle Orthod. 2018 Jan;88(1):27-34. doi: 10.2319/060617-375.1. Epub 2017 Oct 20. PMID: 29053335; PMCID: PMC8315708.
- De Clerck EE, Swennen GR. Success rate of miniplate anchorage for bone anchored maxillary protraction. Angle Orthod. 2011 Nov;81(6):1010-3. doi: 10.2319/012311-47.1. Epub 2011 Jun 30. PMID: 21721948; PMCID: PMC8903855.
- Chung K, Kim SH, Kook Y. C-orthodontic microimplant for distalization of mandibular dentition in Class III correction. Angle Orthod. 2005 Jan;75(1):119-28. doi: 10.1043/0003-3219(2005)075<0119:CMFDOM>2.0.CO;2. PMID: 15747827.
- Chung KR, Kim SH, Choo H, Kook YA, Cope JB. Distalization of the mandibular dentition with mini-implants to correct a Class III malocclusion with a midline deviation. Am J Orthod Dentofacial Orthop. 2010 Jan;137(1):135-46. doi: 10.1016/j.ajodo.2007.06.023. PMID: 20122441.
- Jing Y, Han X, Guo Y, Li J, Bai D. Nonsurgical correction of a Class III malocclusion in an adult by miniscrew-assisted mandibular dentition distalization. Am J Orthod Dentofacial Orthop. 2013 Jun;143(6):877-87. doi: 10.1016/j.ajodo.2012.05.021. PMID: 23726338.
- Poletti L, Silvera AA, Ghislanzoni LT. Dentoalveolar class III treatment using retromolar miniscrew anchorage. Prog Orthod. 2013 May 23;14:7. doi: 10.1186/2196-1042-14-7. PMID: 24325840; PMCID: PMC4384962.
- Chung KR, Kim Y, Choo H, Kim SH, Nelson G. The biocreative strategy. Part 4: Molar distalization in nonextraction treatment. J Clin Orthod. 2018 Sep;52(9):462-475. PMID: 30256221.
- Ye C, Zhihe Z, Zhao Q, Ye J. Treatment effects of distal movement of lower arch with miniscrews in the retromolar area compared with miniscrews in the posterior area of the maxillary. J Craniofac Surg. 2013 Nov;24(6):1974-9. doi: 10.1097/SCS.0b013e3182a248ae. PMID: 24220385.
- Lim JK, Jeon HJ, Kim JH. Molar distalization with a miniscrew-anchored sliding jig. J Clin Orthod. 2011 Jul;45(7):368-77. PMID: 21965317.
- Farret MM, Farret MM, Farret AM. Orthodontic camouflage of skeletal Class III malocclusion with miniplate: a case report. Dental Press J Orthod. 2016 Jul-Aug;21(4):89-98. doi: 10.1590/2177-6709.21.4.089-098.oar. PMID: 27653269; PMCID: PMC5029321.
- Kim SJ, Choi TH, Baik HS, Park YC, Lee KJ. Mandibular posterior anatomic limit for molar distalization. Am J Orthod Dentofacial Orthop. 2014 Aug;146(2):190-7. doi: 10.1016/j.ajodo.2014.04.021. PMID: 25085302.
- Choi YT, Kim YJ, Yang KS, Lee DY. Bone availability for mandibular molar distalization in adults with mandibular prognathism. Angle Orthod. 2018 Jan;88(1):52-57. doi: 10.2319/040617-237.1. Epub 2017 Sep 26. PMID: 28949768; PMCID: PMC8315719.
- Tai K, Park JH, Tatamiya M, Kojima Y. Distal movement of the mandibular dentition with temporary skeletal anchorage devices to correct a Class III malocclusion. Am J Orthod Dentofacial Orthop. 2013 Nov;144(5):715-25. doi: 10.1016/j.ajodo.2012.11.027. PMID: 24182588.
- Tavares CAE, Sheffer MAR, Allgayer S. Surgery first using skeletal anchorage with tandem mechanics for mandibular molar distalization. Am J Orthod Dentofacial Orthop. 2018 Jan;153(1):118-130. doi: 10.1016/j.ajodo.2016.09.035. PMID: 29287638.
- Hu H, Chen J, Guo J, Li F, Liu Z, He S, Zou S. Distalization of the mandibular dentition of an adult with a skeletal Class III malocclusion. Am J Orthod Dentofacial Orthop. 2012 Dec;142(6):854-62. doi: 10.1016/j.ajodo.2011.03.030. PMID: 23195371.