
More Information
Submitted: June 06 05, 2026 | Accepted: June 15, 2026 | Published: June 16, 2026
Citation: Mahajan A, Gera A. Assessment of the Prevalence and Severity of Temporomandibular Joint Disorder Problems in Patients Seeking Orthodontic Treatment: A Cross-Sectional Study. J Clin Adv Dent. 2026; 10(1): 1-6. Available from:
https://dx.doi.org/10.29328/journal.jcad.1001053
DOI: 10.29328/journal.jcad.1001053
Copyright license: © 2026 Mahajan A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Temporomandibular joint; Clicking; Temporomandibular disorders; Fonseca’s questionnaire; Stress; Clicking

Assessment of the Prevalence and Severity of Temporomandibular Joint Disorder Problems in Patients Seeking Orthodontic Treatment: A Cross-Sectional Study
Amanika Mahajan1* and Anmol Gera2*
and Anmol Gera2*
1Dss-258, Sec-20 Panchkula, Haryana, India
213-A Pink city, Peer Muchalla, Zirakpur, India
*Corresponding author: Dr. Amanika Mahajan, Dss-258, Sec-20 Panchkula, Haryana, India, Email: [email protected]
Dr. Anmol Gera, 13-A Pink city, Peer Muchalla, Zirakpur, India, Email: [email protected]
Background and aim: The aim of the study is to assess the prevalence of TMD among patient seeking orthodontic treatment.
Introduction: Temporomandibular disorders are a general term used to describe a subset of orofacial pain syndromes (TMDs). This category involves problems with the temporomandibular joint, weariness in the masticatory muscles, difficulty moving the jaw, and articular noises. TMD is most commonly seen in women than in men and is more prevalent between the ages of 20 and 40.
Materials and method: This descriptive cross-sectional study was done from June 2025 to March 2026 and 250 patients who had visited the outpatient department (OPD) of the Department of Orthodontics and Dentofacial Orthopedics at Yamuna Institute of Dental Sciences and Research, Yamuna Nagar were examined. Of these, 200 patients (100 females and 100 males) were included in the study. The prevalence and severity of TMD was assessed using the Fonseca questionnaire.
Results: The results showed the most frequent symptoms elicited by the participants in this study included clicking in the TMJ during chewing, difficulty in mouth opening, headaches and masticatory pain. Females showed higher prevalence of TMD signs and symptoms than men. Also, there was a greater frequency of symptoms in those who self-reported as stressed.
Conclusion: TMD was common in those with headaches, clicking sounds when opening or chewing, and muscle soreness. The extent of effect on normal daily activity was found to be significantly more among those having severe TMD.
Temporomandibular disorders (TMDs) represent subclass of painful orofacial disorders comprising complaints of discomfort on the temporomandibular joint (TMJ) region commonly referred to as temporomandibular disorders (TMD) [1]. The American Academy of Orofacial Pain defines Temporomandibular Disorders (TMDs) as a “Collective term that embraces a number of clinical problems that involve the masticatory muscles, the TMJ (Temporomandibular joint), and the associated structures” [2].
Temporomandibular disorders are considered multifactorial in origin, arising from the interaction of biological, mechanical, and psychosocial factors. Emotional stress, occlusal interferences, missing teeth, postural deviations, masticatory muscle dysfunction, and structural changes affecting the temporomandibular joint have all been identified as potential contributing factors. Acting alone or in combination, these factors may disrupt the normal functional equilibrium of the stomatognathic system. Consequently, the coordinated relationship among the temporomandibular joints, masticatory muscles, and dental occlusion may be compromised, resulting in the development of temporomandibular disorders [3].
The orthodontic community paid little attention to the TMD sector until the late 1980s, when a lawsuit alleged that orthodontic treatment was directly responsible for a patient’s discomfort. Following the incident, various research objectives were developed to acquire a better understanding of the relationship between TMD and orthodontics. When it comes to orthodontics and TMD, the most common topic of discussion is occlusion. Furthermore, occlusion isn’t the sole possible cause of TMD [4]. According to Okeson, trauma, deep pain input, parafunctional activity, and emotional stress are at least four additional variables that may contribute to TMD. Understanding that these variables are not the only ones that determine whether or not TMD will strike someone. Other factors, including a person’s biology, past experiences, genetics, somatoform comorbid diseases, and psychological conditions, have already been found to be involved in the process [16].
Previous studies have reported a considerable prevalence of temporomandibular disorders (TMD) across different populations. According to Almubarak SM, et al, TMD is more commonly observed in females than males, with prevalence estimates ranging from 3.7% to 12%, and is most frequently seen among individuals aged 20–40 years [3]. Similarly, Nomura, et al. reported that women are affected by TMD nearly nine times more often than men [15]. Furthermore, Schiffman, et al. found that over 50% of the general population exhibit at least one sign of TMD, while more than 30% report one or more related symptoms. The wide variation in reported prevalence rates across studies may be attributed to differences in demographic characteristics, racial and ethnic backgrounds, sampling methods, diagnostic criteria, study designs, and data collection techniques. These findings highlight the multifactorial nature of TMD and the importance of using standardized assessment tools when evaluating its prevalence in different populations [5].
Due to its great prevalence and severity, early diagnosis is critical because it is a progressive disease that, in its late stages, becomes incurable due to TMJ damage. Although a number of measures have been developed for TMD problems, no suitable criteria have been identified. Helkimo [6] popularized the use of anamnestic and clinical indices as there was a need for a simple and trustworthy questionnaire in order to obtain and compare data regarding the severity of TMD from diverse clinical studies [6].
In 1992, Fonseca created an anamnestic questionnaire based on previous indices. The Fonseca’s anamnestic index (FAI) is a self-administered questionnaire that can be used as a low-cost and simple TMD screening tool for non-patients. The Fonseca Questionnaire classified TMD as light, moderate, severe, or non-TMD [5,7]. The advantages of Fonseca’s questionnaire(TMJ Pain Questionnarie) includes short time of application, low cost and less influence from the examiner and less variability in the measures.
Early TMD diagnosis and therapy are crucial, much like with most disorders. The degenerative nature of Temporomandibular dysfunction means that it worsens over time. The variations between different groups and among different demographics are predicted due to the heterogeneous nature of the causes related with TMD. If it is treated in its early phases, the prognosis is favorable. Additionally, early diagnosis and adequate treatment can reduce symptoms and improve the quality of life and safeguarding their health.
Thus, the objective of the study is to assess the prevalence and severity of TMD in patients seeking orthodontic treatment using the Fonseca Anamnestic Questionnaire and to compare the occurrence and severity of TMD between males and females, thereby highlighting the importance of routine screening for temporomandibular disorders during orthodontic assessment and treatment planning.
Study design
This is a descriptive cross-sectional study. The study was conducted from the June 2025 to March 2026. A total of 250 patients of age 18- 30 years who had reported to the OPD of the Department of Orthodontics and Dentofacial Orthopedics of Yamuna Institute of Dental Sciences and Research, Yamuna Nagar were screened. A non-probability consective sampling method with equal gender allocation was used. Out of which 200 patients (100 females & 100 males) were included for the study. The study protocol received approval from the Ethical Committee of Yamuna Institute of Dental Sciences & Research, Yamuna Nagar. Written informed consent was obtained from all participants before participation. All participants were informed about the purpose and procedures of the study, and their participation was voluntary. Confidentiality of the collected data was maintained at all stages of the study.
Sample size estimation
The sample size for the present study was determined based on the prevalence reported in a previous study conducted by Karthik R, et al. [8]. Using the estimated prevalence from the reference study, the required sample size was calculated according to Daniel’s formula for cross-sectional studies:
N = Z2 P(1-P)/d2
where N represents the required sample size, Z is the standard normal deviate corresponding to the desired confidence level, P is the estimated prevalence of the condition under study, and d is the acceptable margin of error (precision). A 95% confidence level (Z = 1.96) and an alpha error of 0.05 were considered for the calculation. Accordingly, a total of 200 patients seeking orthodontic treatment were included in the study to assess the prevalence and severity of temporomandibular disorders and to facilitate gender-wise comparisons.
Inclusion criteria:
Participants in the study comprised both males and females with permanent dentition seeking orthodontic treatment.
Exclusion criteria:
- Patients who didn’t give informed consent
- Patients with primary dentition
- Craniofacial anomalies
- Immunocompromised patients
- Musculoskeletal or neurological disorders
- Non-coperative patients
- Chronic inflammatory pathologies (Rheumatoid Arthritis, Jevenile Idiopathic Arthritis)
The TMD evaluation questionnaire used in this study
Fonseca questionnaire
The Fonseca questionnaire is a pre-validated questionnaire developed by Fonseca and is used to assess the individuals' level of TMD (Table 1). It is 10-item questionnaire used for evaluating the existence of pain in the head, TMJ, and when chewing, parafunctional behaviors, movement restriction, joint clicking, feeling of malocclusion, and emotional strain. TMD was categorized as light, moderate, severe, or non-TMD using the Fonseca questionnaire. The patients were explained about the questionnaire, goals of the research procedures, benefits about early diagnosing and detecting TMDs. The subjects were evaluated for any muscular pain and click while opening and closing the mouth. Questionnaire was done by face to face interview mode.
| Table 1: Fonseca TMJ Questionnaire | |||
| Questions | No | Sometimes | Yes |
| 1. Is it hard for you to open your mouth? | |||
| 2. Is it hard for you to move your mandible from side to side? | |||
| 3. Do you get tired or muscular pain while chewing? | |||
| 4. Do you have frequent headaches? | |||
| 5. Do you have pain on the nape or a stiff neck? | |||
| 6. Do you have earaches or pain in craniomandibular joints? | |||
| 7. Have you noticed any TMJ clicking while chewing or when you open your mouth? | |||
| 8. Do you clench or grind your teeth? | |||
| 9. Do you feel your teeth do not articulate well? | |||
| 10. Do you consider yourself a tense (nervous) person? | |||
The other questions focused on trauma, orthodontic therapy, and any previous TMD treatments. The participants provided the following responses: "yes," "no," and "sometimes." As directed, only one response was to be marked for each question.
This study involved 200 patients (100 females and 100 males). Sex predilection with TMJ disorder was analyzed. Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) software version 14.0 for Windows. The association between variables, including gender and severity of temporomandibular disorders (TMD), was assessed using the Chi-square test. A p - value less than 0.05 (p < 0.05) was considered statistically significant for all analyses.
The present study revealed a positive correlation between TMD and symptoms such as headaches, joint clicking during mastication or mouth opening, stress and nervousness, muscular fatigue or pain during chewing, and parafunctional habits including tooth clenching or grinding (Table 2). A gender-based comparison further demonstrated that the prevalence of TMD was greater among females than males, indicating a higher susceptibility to TMD in female participants (Figure 1).
| Table 2: Gender wise comparison of prevalence of TMJ according Fonseca Questionnaire | ||
| Variables/ Questions | Females % | Males % |
| Is it hard for you to open your mouth? | 11.90% | 6% |
| Is it hard for you to move your mandible from side to side? | 7.9% | 4% |
| Do you get tired/muscular pain while chewing? | 18.8% | 4% |
| Do you have frequent headaches? | 19.80% | 11.10% |
| Do you have pain on the nape or stiff neck? | 14.80% | 11.10% |
| Do you have earaches or pain in craniomandibular joints? | 5% | 6% |
| Have you noticed any TMJ clicking while chewing or when you open your mouth? | 37.60% | 18.20% |
| Do you clench or grind your teeth? | 15.80% | 10.1% |
| Do you feel your teeth do not articulate well? | 9.90% | 8.10% |
| Do you consider yourself a tense (nervous) person? | 23.80% | 9.10% |
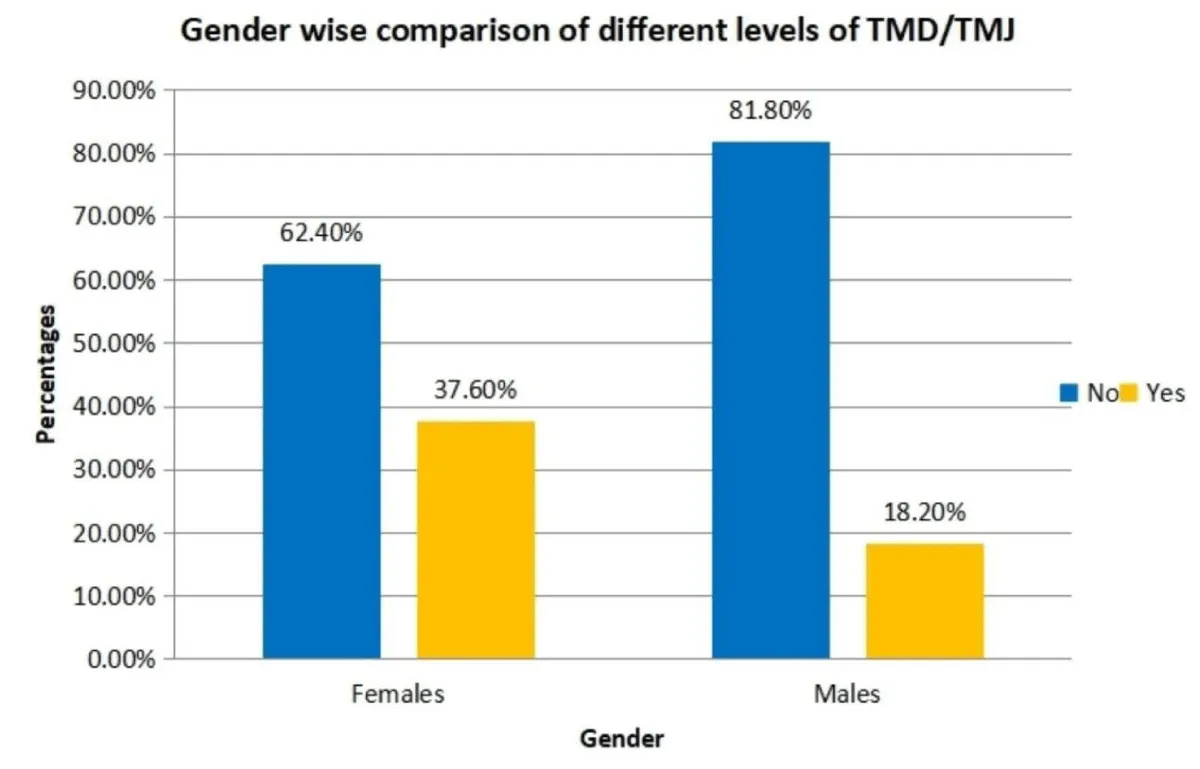
Figure 1: Genderwise comparison of different levels of TMD.
The results of the present study indicated that TMJ clicking, stress and nervousness, masticatory muscle fatigue or pain during chewing, and headaches were significantly associated with temporomandibular disorders among both male and female participants. These symptoms represented the most frequently reported positive responses on the Fonseca Anamnestic Questionnaire. The distribution of positive responses related to TMD symptoms is presented in Figures 2–4. The association between hard to open the mouth, hard to move the mandible from side to side, pain on the nape or stiff neck, earaches or pain in the craniomandibular joints, and teeth that do not articulate well were not found to be statistically significant among males and females in the study.
Bar graph depicting the association between TMJ clicking while chewing or opening of mouth and TMD showed 55.80% of patients had TMJ clicking during chewing or opening the mouth and was the most common symptom seen in patients (Figure 2). The prevalence of TMD was found to be significantly more among those who reported to have click.
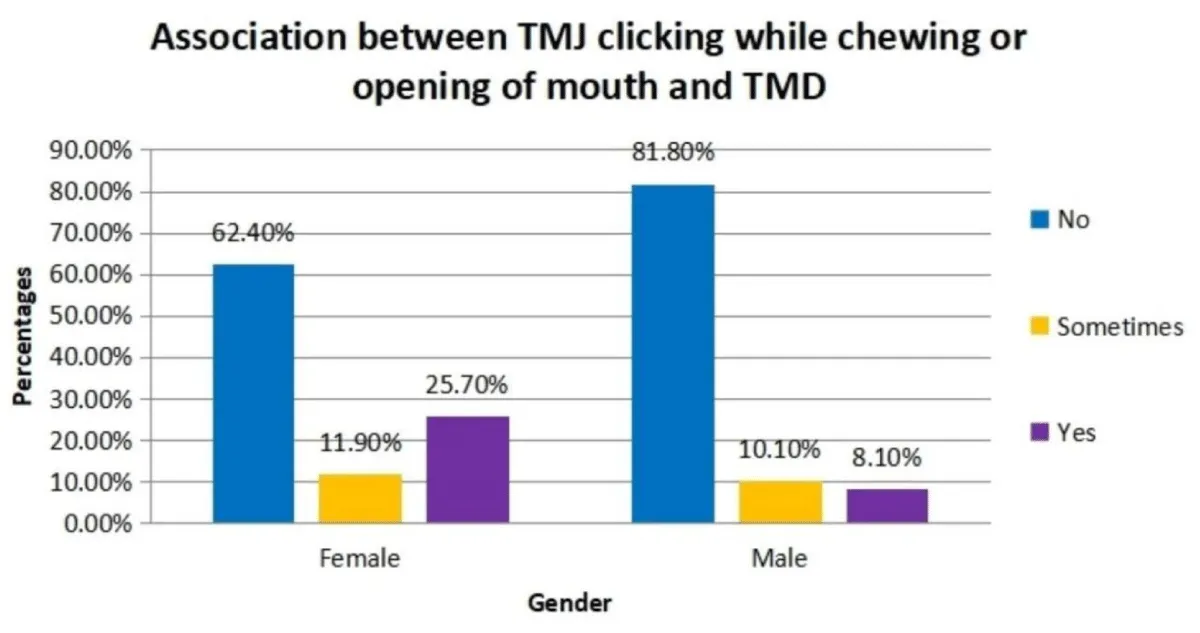
Figure 2: Association between TMJ clicking and TMD.
Association of stress and anxiety with the development of TMD showed 32.90% of patients had positive correlation. Those who reported experiencing occasional or frequent anxiety were found to have a considerably higher prevalence of TMD (Figure 3).
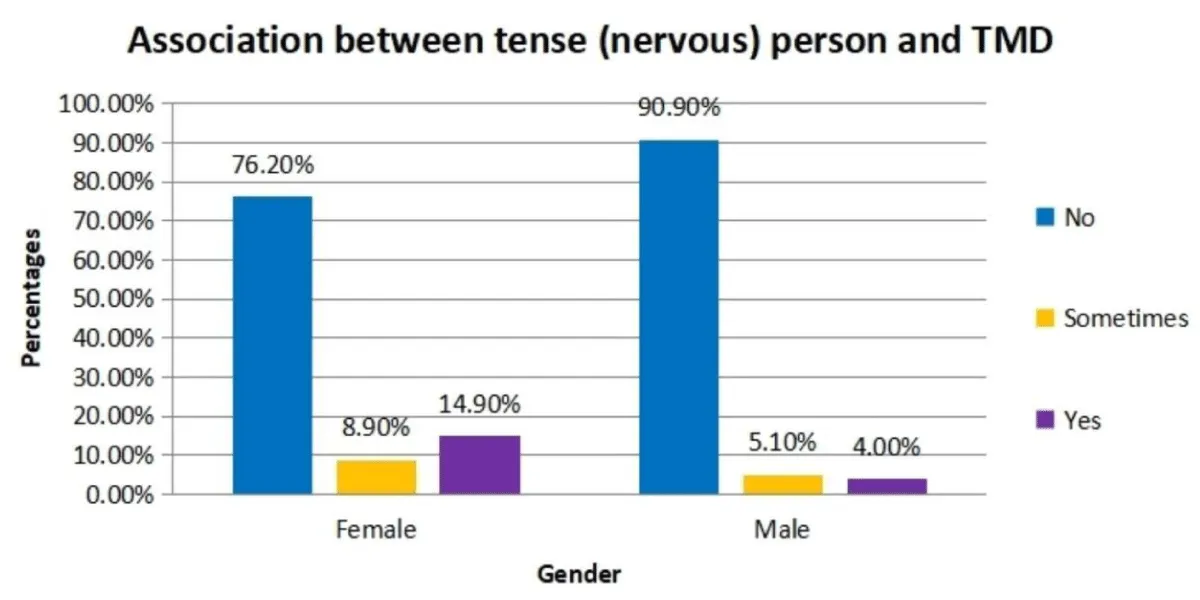
Figure 3: Association between tense person and TMD.
The association between TMD and muscular pain on chewing showed 22.80% of patients had muscular pain while chewing and the prevalence of frequent headaches was found to be significantly associated with the prevalence of TMD. 31.90% of patients reported to have frequent or occasional headaches (Figure 4).
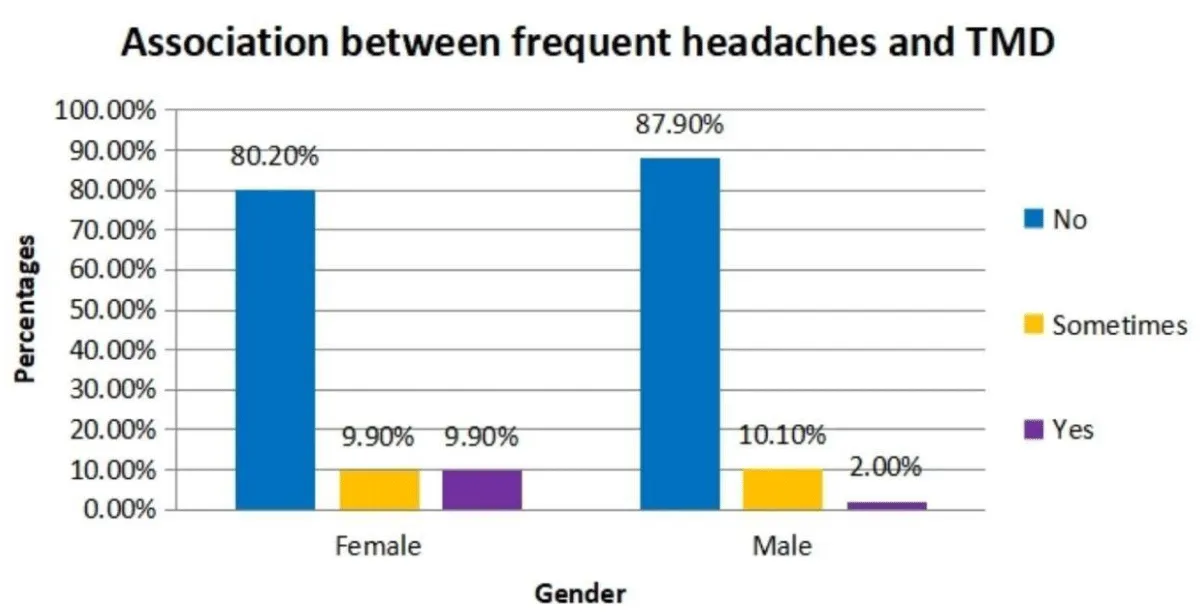
Figure 4: Association between frequent headaches and TMD.
The Temporomandibular joint (commonly referred to as the ginglymoarthrodial joint) comes from the Greek words “arthrodia,” which refers to a joint that allows surfaces to glide, and “ginglymus,” which refers to a hinge joint that only allows motion back and forth in one plane. The diarthrodial bilateral Temporomandibular joints (TMJs) make up the Temporomandibular articulation. A mandibular condyle with the glenoid fossa and articular eminence that correspond to it comprise each joint. The Temporomandibular disorders refers to a subset of painful orofacial disorders that involve pain in the Temporomandibular joint region and masticatory muscle involvement that limits mandibular movements.
The purpose of this study was to assess the frequency of TMD in outpatient department (OPD) of Orthodontics and Dentofacial Orthopedics through frequency distribution of data obtained using a questionnaire. The Fonseca’s questionnaire was used in the study because of its low cost, assures substantial collection of an information in a brief time frame and validity–reliability in its diagnosis making it a valuable instrument for assessing the prevalence and severity of TMDs.
The result of the present study showed the most frequent symptoms elicited by the participants included clicking in the TMJ during chewing (55.8%), difficulty in mouth opening, headaches (31.9%), tooth clenching and grinding (25.8%) and masticatory pain (22.8%) (Table 2). The findings were consistent with earlier research conducted by Valeria Mitro, et al. [18] using Fonseca’s Questionnaire as a tool for carrying out the initial evaluation of Temporomandibular Disorders in dental students [17]. The questionnaire’s data showed that a significant portion of students (78%) displayed symptoms consistent with TMDs. Psychological stress (49.6%), tooth clenching and grinding (34%), joint clicking (33.6%), frequent headaches (15.2%), and neck discomfort (23.2%) were the most commonly reported signs and symptoms. Notably, women were much more affected than men when moderate to severe TMD symptoms were taken into account. Additionally, the prevalence of TMDs did not seem to be influenced by variables like age, work status, or physical activity.
Furthermore, participants who self-reported experiencing stress demonstrated a higher prevalence of TMD-related symptoms (Figure 3). This finding highlights the significant role of psychological factors in the development and progression of temporomandibular disorders. According to Laskin [9], TMD is largely associated with masticatory muscle hyperactivity, emotional stress, and adverse oral habits such as clenching and bruxism. Psychological stress can increase muscle tension and parafunctional activity, leading to muscular fatigue, pain, spasms, and dysfunction of the temporomandibular joint. Prolonged muscle hyperactivity may further contribute to joint instability, disc displacement, and impaired mandibular movements.
The association between stress and TMD has important clinical implications, as emotional stress is considered a major contributing factor in the multifactorial etiology of TMD. Stress-induced alterations in muscle activity can exacerbate existing symptoms and increase the risk of developing temporomandibular dysfunction. Therefore, the assessment of psychological well-being should form an integral part of TMD evaluation and management. Incorporating stress reduction strategies, behavioral modification, and patient counseling may help improve treatment outcomes and reduce symptom severity.
The results were in accordance with the previous investigations done by Kanehira H, et al. [10], Yamaguchi D, et al. [11], Ebrahimi M, and Choudhary Sh, et al. [12,13] that reported a significant relationship between emotional stress and TMD. These studies suggested that psychological stress can influence neuromuscular function, alter masticatory muscle activation patterns, and increase susceptibility to temporomandibular disorders. Collectively, the evidence supports the view that stress is not merely a secondary consequence of TMD-related pain but may also act as a contributing etiological factor in the onset and progression of the disorder.
Kanehira H, et al. [10] found the association between stress and temporomandibular disorders and concluded that stress had a substantial correlation with serious TMD symptoms and parafunction. Psychological factors, including stress, have a significant influence in TMD. Yamaguchi D, et al. [11] evaluated the psychological aspects in orthodontic patients with TMD using the “TMJ scale” and found that female patients in the symptom group showed a higher degree of stress due to chronic pain and anomalies in the TMJ than those in the non-symptom group. Choudhary Sh, et al. [13] designed an institutional survey to evaluate dentistry students’ knowledge and self-awareness regarding temporomandibular joint diseases and concluded that psychological elements like stress may play a part in TMD development and there was a progressive increase in TMD indications and symptoms with higher academic educational levels.
Kariny Nomura, et al. [15]. evaluated the frequency and severity of Temporomandibular problems among Brazilian dental undergraduates using Fonseca’s questionnaire and concluded that 53.21% showed some level of TMD: 35.78% mild TMD 11.93% moderate and 5.5% severe TMD and women had higher prevalence among males. In the similar study by Karthik R, et al. [8] investigated the frequency of Temporomandibular issues among university students and concluded that female predominance was seen, with increasing prevalence among tense patients, and there was a strong association between the existence of TMDs and a history of trauma.
Another study, conducted by Prashantha G Shivamurthy, et al. [14], examined the prevalence and severity of temporomandibular disorders (TMD) among college students using the Fonseca Anamnestic Questionnaire. The authors found that 33.3% of subjects had TMD symptoms ranging from mild to severe dysfunction. The data revealed that a sizable proportion of young adults have TMD-related signs and symptoms, even in the lack of a definitive diagnosis. The study emphasized the Fonseca Questionnaire’s usefulness as a simple and effective screening tool for identifying individuals at risk of TMD, as well as the importance of early detection and preventive measures among college-going populations to reduce TMD’s potential impact on oral function and quality of life.
In the present study, TMD was common in those with headaches, clicking sounds when opening or chewing, and muscle soreness. TMD signs and symptoms are more prevalent in females than in males. Individuals who reported experiencing stress and anxiety on a regular or infrequent basis had a greater incidence of TMD [19-22].
The present study assessed the prevalence and severity of temporomandibular disorders (TMD) using the Fonseca Questionnaire and identified several factors associated with the condition. Participants reporting recurrent headaches, temporomandibular joint clicking during chewing or mouth opening, and masticatory muscle soreness were found to have a higher likelihood of experiencing TMD. Furthermore, individuals with severe TMD reported a significantly greater impact on their daily activities, highlighting the substantial functional burden associated with advanced disease severity.
The findings also demonstrated a higher prevalence of TMD symptoms and signs among females compared with males. In addition, self-reported psychological stress was positively associated with the presence and severity of TMD symptoms, suggesting a potential role of psychosocial factors in the development and progression of the disorder.
Overall, these results emphasize the multifactorial nature of TMD and the importance of early identification of clinical symptoms and contributing risk factors. Increased awareness, timely diagnosis, and comprehensive management strategies addressing both physical and psychological aspects may help reduce the impact of TMD on patients’ quality of life.
Limitations
The cross-sectional design limits the ability to establish causal relationships between the identified risk factors and temporomandibular disorders (TMD). As data were collected at a single point in time, it was not possible to determine whether the observed symptoms and associated factors preceded the development of TMD or resulted from the disorder itself. Furthermore, the study could not assess changes in symptom severity, disease progression, or fluctuations in clinical manifestations over time.
The use of a questionnaire-based assessment may also have introduced response and recall bias, as participants’ responses were dependent on their subjective perception and recollection of symptoms. Although the Fonseca Questionnaire is a widely accepted screening tool for TMD, it does not provide a definitive clinical diagnosis and should ideally be complemented by comprehensive clinical and radiographic evaluations.
Financial support and sponsorship: The study was self-funded, and no external financial support or sponsorship was received.
Conflict of interest: The authors declare that there are no conflicts of interest related to this study.
Author contributions
The authors contributed equally to the conception and design of the study, data collection, data acquisition, statistical analysis, and interpretation of the results. They were also involved in the preparation, critical revision, and final review of the manuscript. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Acknowledgment
The authors gratefully acknowledge the support and valuable contributions of their colleagues, whose guidance and expertise greatly assisted in the conduct of this study.
- Shivamurthy PG, Kumari N, Sadaf A, Meghana MB, Azhar H, Sabrish S. Use of Fonseca’s Questionnaire to assess the prevalence and severity of Temporomandibular disorders among university students-a cross sectional study. Dentistry 3000. 2022 Feb 25;10(1).
- Porto F, Harrell R, Fulcher R, Gonzales T. Knowledge and beliefs regarding temporomandibular disorders among orthodontists. American Journal of Orthodontics and Dentofacial Orthopedics. 2019 Oct 1;156(4):475-84. Available from: https://doi.org/10.1016/j.ajodo.2018.10.022
- Almubarak SM, Ashour LM, Hussein Z, Aleissa AM, Mortaga RM, Al Khulaifi RK, et al. Current Concepts About Temporomandibular joint disorders: A Review. Journal of Research in Medical and Dental Science. 2020 Nov;8(7):471-9.
- Porto F, Harrell R, Fulcher R, Gonzales T. Knowledge and beliefs regarding temporomandibular disorders among orthodontists. American Journal of Orthodontics and Dentofacial Orthopedics. 2019 Oct 1;156(4):475-84. Available from: https://doi.org/10.1016/j.ajodo.2018.10.022
- Schiffman EL, Fricton JR, Haley DP, Shapiro BL. The prevalence and treatment needs of subjects with temporomandibular disorders. J Am Dent Assoc. 1990;120:295–303. Available from: https://doi.org/10.14219/jada.archive.1990.0059
- Helkimo M. Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Sven Tandlak Tidskr 1974;67:101-21. Available from: https://pubmed.ncbi.nlm.nih.gov/4524733/
- Fonseca DM. Craniomandibular Dysfunction (DCM): Diagnosis by the Anamnesis [Master's Dissertation]. Bauru: Faculty of Dentistry of Bauru of USP; 1992.
- Karthik R, Hafila MF, Saravanan C, Vivek N, Priyadarsini P, Ashwath B. Assessing prevalence of temporomandibular disorders among university students: a questionnaire study. Journal of international society of preventive and community dentistry. 2017 Jun 1;7(Suppl 1):S24-9. Available from: https://doi.org/10.4103/jispcd.jispcd_146_17
- Laskin DM. Etiology of the pain-dysfunction syndrome. J Am Dent Assoc 1969; 79: 147–153. Available from: https://doi.org/10.14219/jada.archive.1969.0234
- Kanehira H, Agariguchi A, Kato H, Yoshimine S, Inoue H. Association between stress and temporomandibular disorder. J Jpn Prosthodont Soc 2008;52:375-80. Available from: https://doi.org/10.2186/jjps.52.375
- Yamaguchi D, Motegi E, Nomura M, Narimiya Y, Katsumura S, Miyazaki H, et al. Evaluation of psychological factors in orthodontic patients with TMD as applied to the “TMJ scale” Bull Tokyo Dent Coll. 2002;43:83–7. Available from: https://doi.org/10.2209/tdcpublication.43.83
- Ebrahimi M, Dashti H, Mehrabkhani M, Arghavani M, Daneshvar-Mozafari A. Temporomandibular disorders and related factors in a group of Iranian adolescents: a cross-sectional survey. Journal of dental research, dental clinics, dental prospects. 2011;5(4):123. Available from: https://doi.org/10.5681/joddd.2011.028
- Choudhary SH, Kale LM, Mishra SS, Sodhi S, Muley PB, Pandey ND. An institutional survey for knowledge-based and self-awareness assessment in temporomandibular joint disorders among dental students. Indian Journal of Dental Research. 2016 May 1;27(3):262-7. Available from: https://doi.org/10.4103/0970-9290.186238
- Shivamurthy PG, Kumari N, Sadaf A, Meghana MB, Azhar H, Sabrish S. Use of Fonseca’s Questionnaire to assess the prevalence and severity of Temporomandibular disorders among university students-a cross sectional study. Dentistry 3000. 2022 Feb 25;10(1). Available from: https://doi.org/10.1590/s0103-64402007000200015
- Nomura K, Vitti M, Oliveira AS, Chaves TC, Semprini M, Siéssere S, et al. Use of the Fonseca's questionnaire to assess the prevalence and severity of temporomandibular disorders in Brazilian dental undergraduates. Brazilian dental journal. 2007;18:163-7. Available from: https://doi.org/10.1590/s0103-64402007000200015
- Jeffrey P. Okeson Management of Temporomandibular disorders and Occlusion. 7 edition.
- De Oliveira AS, Dias EM, Contato RG, Berzin F. Prevalence study of signs and symptoms of temporomandibular disorder in Brazilian college students. Braz Oral Res 2006;20:3-7. Available from: https://doi.org/10.1590/s1806-83242006000100002
- Mitro V, Caso AR, Sacchi F, Gilli M, Lombardo G, Monarchi G, et al. Fonseca’s questionnaire is a useful tool for carrying out the initial evaluation of temporomandibular disorders in dental students. Clinics and Practice. 2024 Aug 26;14(5):1650-68. Available from: https://doi.org/10.3390/clinpract14050132
- Bonjardim LR, Gavião MB, Pereira LJ, Castelo PM, Garcia RC. Signs and symptoms of temporomandibular disorders in adolescents. Braz Oral Res 2005;19:93-8. Available from: https://doi.org/10.1590/s1806-83242005000200004
- Schiffman E, Fricton JR. Epidemiology of TMJ and craniofacial pain: Diagnosis and management. In: Kraus SL, editor. The TMJ Disorders Management of the Craniomandibular Complex. New York: Churchill Livingstone; 1998. p. 23-38.
- Habib SR, Al Rifaiy MQ, Awan KH, Alsaif A, Alshalan A, Altokais Y. Prevalence and severity of temporomandibular disorders among university students in Riyadh. Saudi Dent J 2015;27:125-30. Available from: https://doi.org/10.1016/j.sdentj.2014.11.009
- Pedroni CR, De Oliveira AS, Guaratini MI. Prevalence study of signs and symptoms of temporomandibular disorders in university students. J Oral Rehabil 2003;30:283-9. Available from: https://doi.org/10.1046/j.1365-2842.2003.01010.x